Automatisation of catheter reconstruction in interstitial breast BT using electromagnetic tracking
Christopher Dürrbeck,
Germany
OC-0631
Abstract
Automatisation of catheter reconstruction in interstitial breast BT using electromagnetic tracking
Authors: Christopher Dürrbeck1, Nadin Abu-Hossin1, Michael Lotter1, Stephan Kreppner1, Dorota Lubgan1, Rainer Fietkau1, Vratislav Strnad1, Christoph Bert1
1Universitätsklinikum Erlangen, Department of Radiation Oncology, Erlangen, Germany
Show Affiliations
Hide Affiliations
Purpose or Objective
Catheter reconstruction is the most time-consuming step
of treatment planning for interstitial catheter implants in breast
brachytherapy. The manual reconstruction time is typically 3-5 minutes per
catheter, adding up to an hour or more for the whole implant. Besides that, it
is prone to systematic human errors. The objective of this work was to evaluate
the capabilities of an electromagnetic tracking (EMT) system integrated into an
afterloader for automated online catheter reconstruction.
Material and Methods
An afterloader prototype (Flexitron, Elekta Brachytherapy,
Veenendaal, The Netherlands) equipped with an EMT sensor was used to assess the
geometry of the catheter implant of 20 patients immediately after the planning
CT with the patient still on the CT couch. The acquired EMT data were processed
and registered to the clinically used, manual catheter reconstruction which
served as a ground truth. In the future the registration is to be done based on
the fixation buttons as mutual landmarks. For this reason, an approach to
detect the buttons using EMT and tiny embedded magnets is also currently
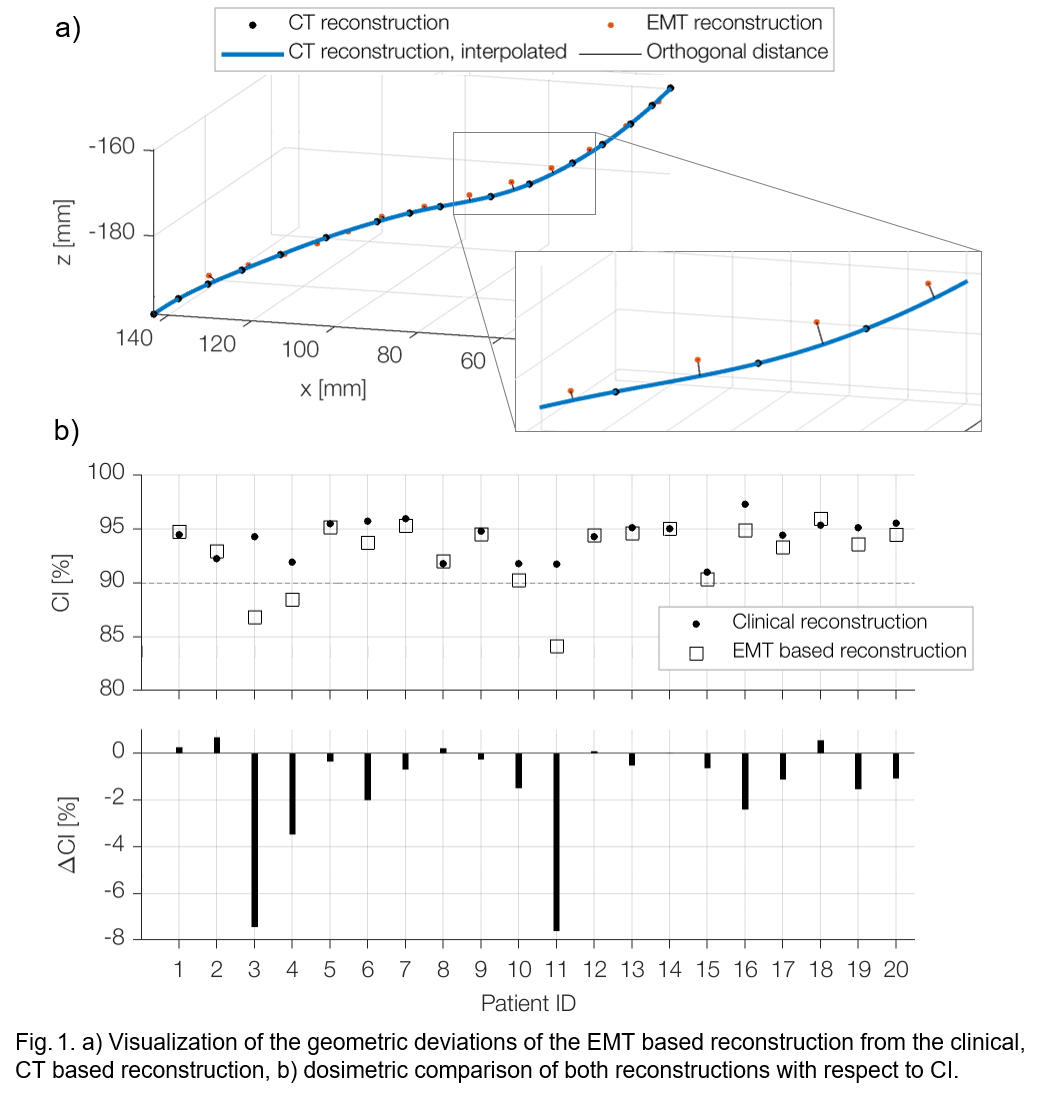
investigated. The geometric reconstruction accuracy was determined as the
minimum orthogonal distance of an EMT reconstruction point to the clinical
catheter path (Fig. 1, a). For dosimetric evaluation the EMT reconstructions
were imported into the research version of the treatment planning system Oncentra
Brachy (Elekta Brachytherapy, Veenendaal, The Netherlands), along with the
clinically approved structure set and treatment plan including dwell positions
and dwell times. Standard figures of merit (CI, DNR, and COIN) were calculated
in order to appraise the quality of the implant.
Results
The acquisition time of the EMT system is 22 s per
catheter and typically 6-11 min for the entire implant, the time for data
processing is < 1 min. The median distance between EMT
reconstruction points and clinical reconstruction is 1.1 mm with an
interquartile range of 1.1 mm. The median CI decreased from 94.7 % for the
clinical reconstruction to 94.1 % for the EMT based reconstruction while both
the median DNR (0.24) and the median COIN (0.69) did not change. However, in two
individual patients a drop of the CI as large as 7.5 % could be observed
(Fig. 1, b). In three cases the CI was < 90 %. None of the implants failed
the requirements for maximum skin dose.
Conclusion
The EMT based implant reconstruction was found to be geometrically
accurate within the intrinsic limits of the EMT system and did not deteriorate
the dosimetric implant quality in 17 of 20 patients. In the three cases in
which the implant quality decreased, only small manual adjustments of some of
the reconstruction points were sufficient to meet the clinical dose
requirements again. Therefore strategies to further refine the EMT based
reconstruction are currently being explored.