Simulation of interstitial multi-catheter breast brachytherapy using a 3D surface imaging system
Philippe BOISSARD,
France
OC-0630
Abstract
Simulation of interstitial multi-catheter breast brachytherapy using a 3D surface imaging system
Authors: Frédéric GASSA1, Anne-Agath SERRE2, Pascal Pommier3, Aurore Seneclauze3, Sandrine Mancini2
1Centre Leon BERARD, radiotherapy, LYON, France; 2Centre Leon BERARD, radiotherapy, Lyon, France; 3Centre Leon BERARD, Radiotherapy, Lyon, France
Show Affiliations
Hide Affiliations
Purpose or Objective
Brachytherapy for
breast cancer involves positioning several
catheters through the skin into the breast tissues around the lumpectomy site. In order to get an acceptable dose
distribution, the planning target volume (PTV) has to be geometrically covered
by the catheters implanted.
To plan the correct positions and reduce uncertainty between virtual and
final implants, we developed a virtual simulation using Surface Guided
Radiotherapy (SGRT) Technology. We propose to focus on the technical aspects of
this new method.
Material and Methods
On the pre-implant CT, we delineated the PTV according to
GEC ESTRO recommendations. A 3D virtual implant simulation of the catheters
positions was performed using Monaco treatment planning system (Elekta AB,
Stockholm) (TPS). For each virtual catheter, we
created an external beam to obtain the isocenter. Markers were placed on all
entry and exit points. We exported all the informations to a 3D surface patient
setup system for alignment AlignRT® (VisionRT, London) and to record
and verify the system (Mosaiq).
In a radiotherapy
treatment room equipped with AlignRT, we identified and marked on the skin all
entry and exit points using the light field simulator of the linac. AlignRT
assessed real‐time
patient positioning by comparison to a reference surface (patient external
contour of the CT scan).The use of surface imaging could improve the
reproducibility and accuracy of patient positioning with pre scan and reduce uncertainty
in catheter simulation. At the end of this operation, Radiopaque skin markers were
thereafter positioned on the breast surface on the entry and exit points. A CBCT
was performed and exported to the TPS. We performed a registration between the CBCT
and the pre implant CT using surgical scar and clips. The position
of the markers was compared to entrance and exit points. Implantation was then
carried out under local anaesthetic using skin marks of the catheter inlets and
outlets. Final dosimetry was performed on post-implantation CT scan.
Results
For 4
patients, we compared coordinates form the entry and exit points defined on the
pre scan and the CBCT (figure1) to evaluate the accuracy of the simulation.
Mean differences observed were 0.2±0.3cm, 0.2±0.2cm and 0.3±0.4cm in
left-right, supero-infero and antero-posterior (AP), respectively. A maximum
difference of 1.1cm was obtained in the AP direction for external entry points.
The obliqueness of the patient in this area amplified the shift
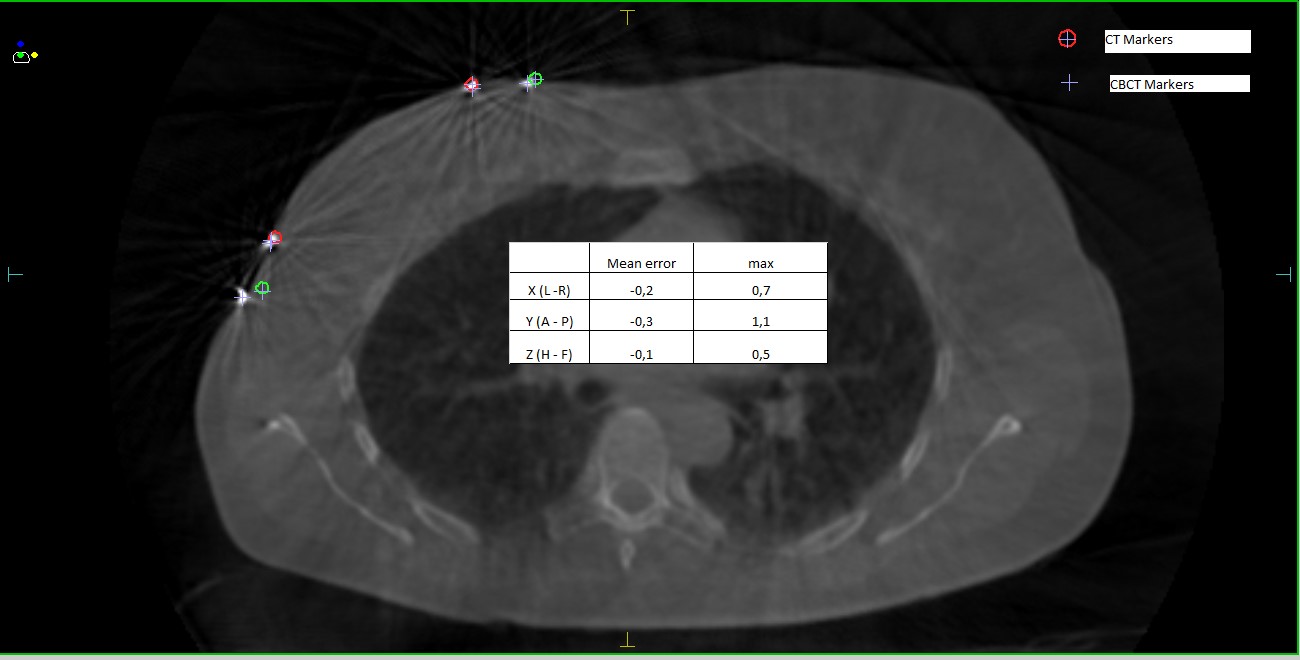
Figure 1:
CBCT obtained after catheters simulation
Conclusion
Assessment
of target volume coverage between the virtual implant and the CBCT showed a
good correlation.
We
concluded that 3D virtual brachytherapy using AlignRT may offer an improved
technique to accurately perform interstitial implants of the breast in selected
patients. Although preliminary results show excellent coverage of the target
volume, additional patients will be required to establish the reproducibility
of this technique and its practical limitations.