Risk factors of radiation pneumonitis in modern adaptive radiotherapy
Christina Maria Lutz,
Denmark
PD-0664
Abstract
Risk factors of radiation pneumonitis in modern adaptive radiotherapy
Authors: Christina Maria Lutz1, Ditte Sloth Møller1, Ane Appelt2,3, Markus Alber4, Lone Hoffmann5, Azza Ahmed Khalil5, Marianne Ingerslev Holt5, Maria Kandi5, Hjørdis Hjalting Schmidt5, Marie Tvilum5, Marianne Marquard Knap5
1Aarhus University Hospital, Department of Oncology, Aarhus N, Denmark; 2University of Leeds, Leeds Institute of Medical Research at St James's, Leed, United Kingdom; 3St James's University Hospital, Leeds Cancer Centre, Leeds, United Kingdom; 4Heidelberg University Hospital, Heidelberg Institute for Radiation Oncology (HIRO), Heidelberg, Germany; 5Aarhus University Hospital, Department of Oncology, Aarhus, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
To fit
radiation pneumonitis (RP) models to two patient cohorts treated at the same
clinic with different RT treatments and compare the risk factors related to the
incidence of RP. To compare the predictability of each model in the other
cohort.
Material and Methods
We included
patients consecutively treated with 50-66Gy in 25-33 fractions (433 pts
2010-2017). In April 2013, the daily online positioning strategy was changed
from match on the vertebrae to match on the primary tumour. Combined with an
adaptive radiotherapy (ART) strategy, this reduced PTV volumes significantly. The
patients were split in two groups: Treated with ART (253 pts, ART group) or before ART
was introduced (180 pts, preART group). Basic characteristics (age, gender, smoking
status, histology, stage (AJCC, 7thEd), performance status (PS)), chronic
obstructive pulmonary disease (COPD), chemotherapy, previous surgery and RT
treatment (GTV volume, mean dose to lungs (MLD) and heart (MHD)). RP was
evaluated retrospectively (CTCAE v3.0), dated at maximum observed RP grade. Separate
multi-variable Cox proportional hazard models were fitted to each group. The
performance of each model in both groups was investigated graphically by
calibration plots (six subgroups, equal size, based on predicted probabilities
180 days after RT start).
Results
Patient
characteristics in the two groups were not significantly different. However, treatment
changed significantly. The use of concomitant chemotherapy (64 % vs 78 %,
p<0.001) and IMRT (86 % vs 100 %, p<0.001) increased, median PTV volume (473
cm3 vs 272 cm3, p<0.001), median MLD (16.4 Gy vs 12.1 Gy, p<0.001) and
MHD (8.0 Gy vs 4.5 Gy, p<0.001) decreased. Fig1 shows the HRs for the preART
and ART model. The effect size of MLD was equal in both models, but non-significant
in ART (both HR=1.53, p=0.009 preART, p=0.094 ART), while a nonsignificant dose
effect for MHD was observed only in the ART model (HR= 1.25, p=0.072). Patients
treated post-operatively (HR=3.13, p=0.041) or for recurrence after surgery (HR=2.94
(p=0.006)) had a significantly higher risk in preART, but both were non-significant
in ART. Patients treated with sequential chemotherapy had a significantly
higher risk (HR=5.45, p=0.017) in ART, but were non-significant in pre-ART. The
predicted probabilities in both models fit the data set they originated from
(Fig2). However, the preART model overestimated the probability in the ART
group, and the ART model underestimated the probability in the preART group, except
for a group of patients with very high predicted probabilities.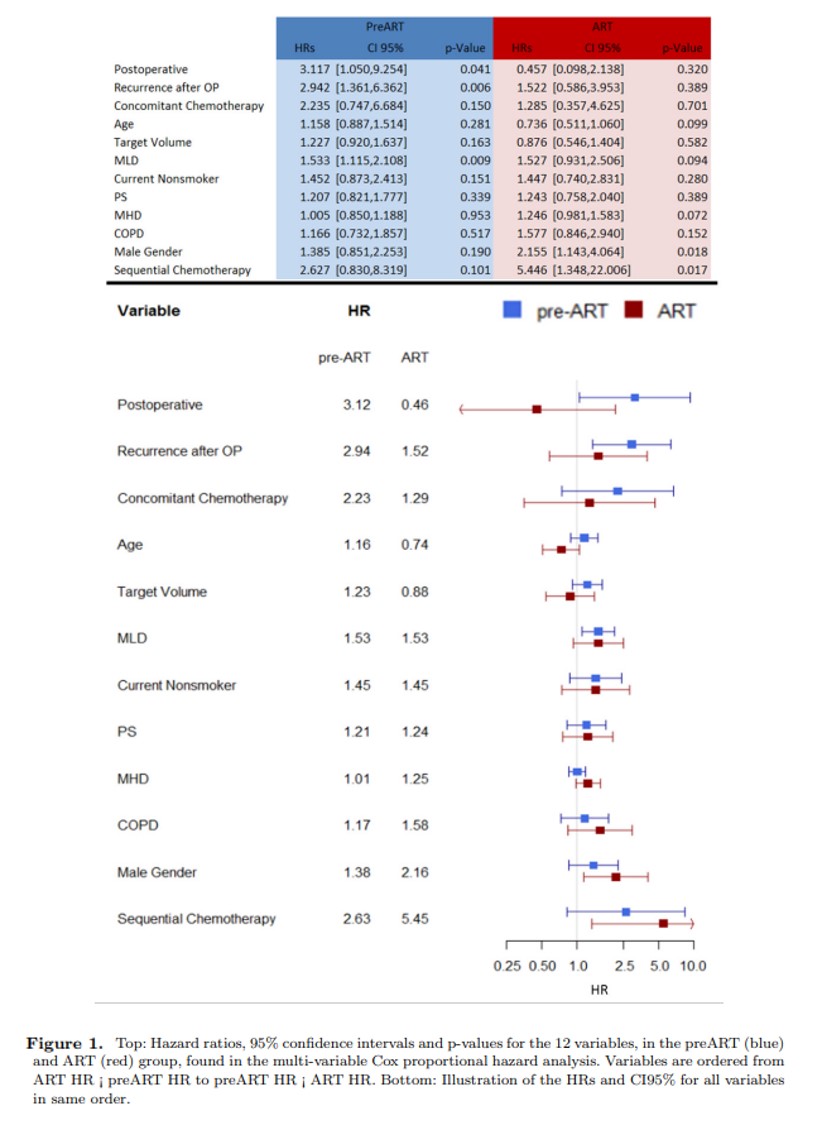

Conclusion
The effect of
lung dose response was constant across the two groups. Other variables, such as
surgery and chemotherapy presented larger variations. While the models fit the
cohort they originate from well, they over/underestimated the probability of RP
in the respective other cohort. This was possibly caused by the underlying
changes in treatment strategies, or by patient selection, and highlights the need
for continuous model adaption.