Contouring lumbosacral plexus based on MR neurography and MR/CT deformable registration technique
PD-0316
Abstract
Contouring lumbosacral plexus based on MR neurography and MR/CT deformable registration technique
Authors: Xi Cao1, Xianshu Gao1, Wei Li2, Peilin Liu3, Shangbin Qin1, Hongzhen Li1, Dian Wang4
1Peking University First Hospital, Radiation oncology, Beijing, China; 2Peking University First Hospital, Radiation department, Beijing, China; 3Peking University First Hospital, Radiation oncology, Beijing , China; 4Rush University Medical Center, Radiation oncology, Chicago, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Traditional image techniques such as nonspecialized MR (layer thickness of 5mm and above) do not perform well in assisting nerve contouring on simulation CT, especially the nerves in the lumbosacral plexus, which have complicated anatomy and are greatly affected by spinal curve changes. We investigated the feasibility of using specialized MR neurography (MRN) and MR/CT deformable registration technique to develop a method for contouring the lumbosacral plexus (LSP).
Material and Methods
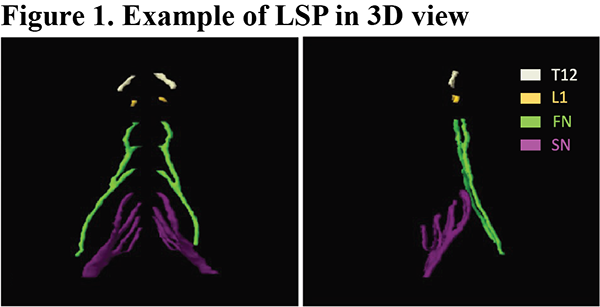
The LSP structure in this study was defined as a combination of the T12 nerve root, L1 nerve root, L2-L4 nerve roots plus femoral nerve (FN), and the L5-S3 nerve roots plus sciatic nerve (SN). Specialized MRN sequences were reviewed, and the NerveVIEW sequence with layer thickness of 2 mm was selected in this study. NerveVIEW sequence were prospectively collected in 18 prostate cancer patients who planned to receive high dose irradiation and one volunteer who completed the carbon ion therapy of her extremity sarcoma in 2017 and subsequently developed radiation-induced lumbosacral plexopathy (RILSP) one year later. Deformable registration was applied to the NerveVIEW sequence and simulation CT images to get fused MR/CT images, on which the LSP was delineated. A dosimetric analysis was done on the enrolled cases with their original treatment plan.
Results
The LSP structures were successfully created in all enrolled patients. In the patient cohort, the mean volume of LSP, FN and SN were 52.7 ± 6.5 cm3 (range, 41.44 – 68.2 cm3), 17.5 ± 3.2 cm3 (range, 13.2 - 23.5 cm3) and 33.4 ± 3.7 cm3 (range, 27.0 – 42.0 cm3), respectively. The median maximal dose to LSP was 52.72 Gy. Three patients received dose excessing 60 Gy to the LSP and two patients received dose excessing 66 Gy. As for the volunteer, the relative biological equivalent maximal dose to her femoral nerve was 67.5 GyE, with V60 at 50.4% and V66 at 34.3%. This high dose to her femoral nerve corresponded to her femoral nerve injury.

Conclusion
We developed a new method for LSP contouring based on specialized MRN and MR/CT deformable registration technique. The preliminary dosimetric analysis has shown that LSP can receive doses exceeding historical and current recommendations if left unattended. This work will shed light on future dosimetric and clinical studies concerning LSP protection.