Artificial intelligence organ-at-risk dose prediction for high-risk prostate cancer IMRT
PD-0322
Abstract
Artificial intelligence organ-at-risk dose prediction for high-risk prostate cancer IMRT
Authors: Patrik Brodin1, Pawas Shukla2, Matthew Hauze2, Leslie Shulte3, Colin Carpenter4, Raman Kumar2, William Bodner2, Shalom Kalnicki2, Madhur Garg2, Wolfgang Tomé1
1Albert Einstein College of Medicine and Montefiore Medical Center, Radiation Oncology, Bronx, USA; 2Montefiore Medical Center, Radiation Oncology, Bronx, USA; 3SIRIS Medical, Dosimetry, Newburyport, USA; 4SIRIS Medical, Research and development, Newburyport, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
To validate the dose prediction performance of a machine learning artificial intelligence (AI) algorithm trained to estimate organ-at-risk (OAR) doses from prostate IMRT using only the planning CT with target and OAR contours. We also investigated the use of these dose predictions to inform planning decisions in a blinded re-planning study.
Material and Methods
Machine learning AI models were trained using a gradient-boosted regression tree algorithm with regularized feature selection based on 105 patients previously treated for high-risk prostate cancer with 45 Gy to the pelvis, 54 Gy to the seminal vesicles and 77.4 Gy to the prostate in 1.8 Gy sequential boost fractions. Fifteen new patients not included in the training set were used to test the OAR dose prediction performance. The same patients were also utilized to generate blinded re-plans with access to the OAR dose predictions but without access to the clinically delivered plans, with target coverage set to meet the same clinical standards. Differences between predicted and delivered doses were assessed by root-mean square deviation (RMSD) and OAR doses comparing predictions, delivered plans and blinded re-plans were evaluated using one-way ANOVA tests.
Results
Prediction performance was excellent with ANOVA tests showing no significant differences between prediction, delivered and re-planned OAR doses (all p-values>0.25, Table 1). Figure 1 shows the comparison between all three scenarios with very close agreement for bladder, rectum and small bowel doses. The RMSD shows low average uncertainty in predicted vs. delivered doses except for Sigmoid V45Gy. The mean difference shows that blinded re-plans achieved OAR doses very close to the clinically delivered plans, with lower small bowel V45Gy, rectum V75Gy and bladder V75Gy in the re-plans for 10/15, 7/15 and 5/15 cases, respectively.
Table 1. Dose prediction root-mean square deviation (RMSD) and difference between delivered treatment plans and blinded re-plans for all organs-at-risk.
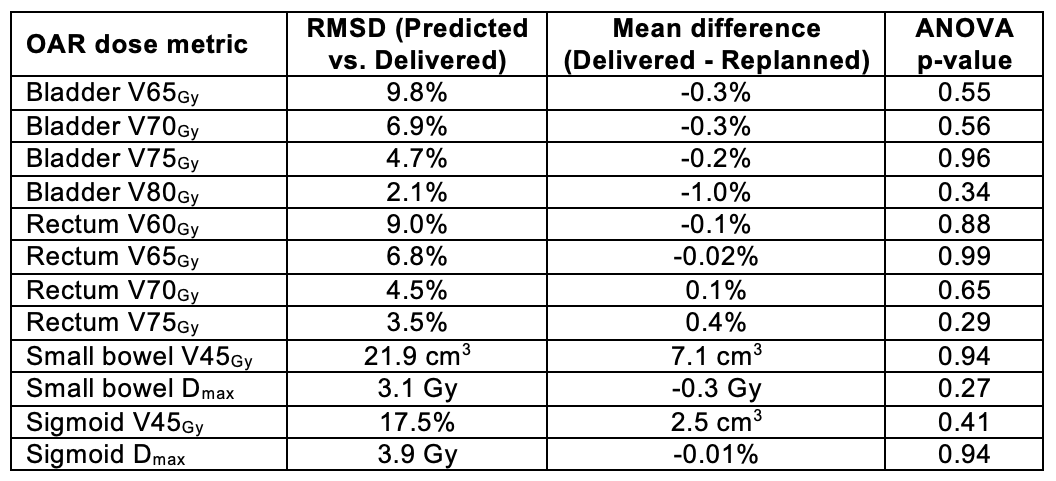
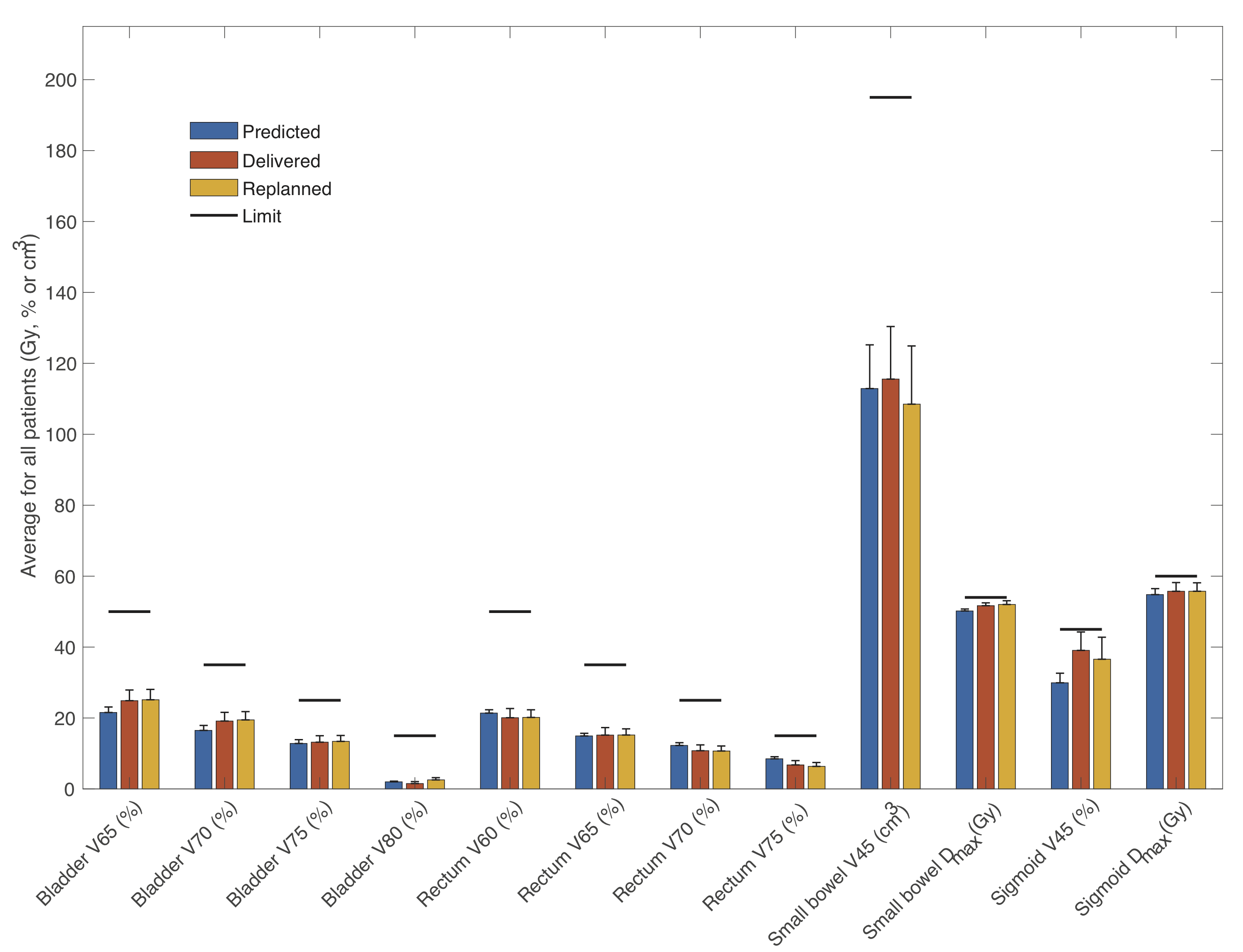
Figure 1. Average DVH dose metric estimates with standard error (vertical error bars) and dose constraint limits (horizontal bars).
Conclusion
Prediction of OAR doses based on planning CT contours showed excellent agreement with delivered prostate IMRT plans and blinded re-plans. Pre-planning access to these dose estimates lead to lower OAR doses for several patients when re-planned. Importantly, estimates of OAR doses prior to initiating the planning process will allow upfront discussions of achievable doses and patient-specific trade-offs, saving time and providing an opportunity for more efficient communication between planner and treating physician.