AI-based auto-segmentation: advantages in delineation, absorbed dose-distribution and logistics
Gustavo R. Sarria,
Germany
PO-1662
Abstract
AI-based auto-segmentation: advantages in delineation, absorbed dose-distribution and logistics
Authors: Gustavo R. Sarria1, Fabian Kugel1, Julian Layer1, Cas Dejonckheere1, Davide Scafa1, Fred Roehner1, Leonard C. Schmeel1
1University Hospital Bonn, Radiation Oncology, Bonn, Germany
Show Affiliations
Hide Affiliations
Purpose or Objective
To compare manually and automatically generated organs at risk and target volume segmentations, in terms of precision and time consumption, based on a retrospective analysis of the absorbed dose distribution of previously delivered VMAT plans.
Material and Methods
The OARs and target volumes from 50 completed VMAT series (25 breast and 25 prostate malignancies) were retrospectively segmented, automatically using the AI-based software Limbus Contour (Limbus AI Inc., Canada) and manually corrected (AI-C) for clinical applicability. The same expert additionally created manually contoured structure sets, which were taken as gold standard (GS-C) based on ESTRO contouring guidelines. All three segmentation strategies were compared geometrically and dosimetrically by calculating Dice coefficients and evaluating clinically relevant absorbed dose limits on both available structure sets. The absorbed dose distributions of the original irradiation plan are used for this purpose. Furthermore, the time differences between approaches are reported.
Results
An overall high correlation rate between OARs and target structures was found for both thoracic and pelvic sites. The DICE coefficient between AI-C and GS-C showed no statistically significant differences for most structures including targets, excepting the contralateral breast, bowel loops, anus and spinal canal (p<0.05). Although not significant, clinically relevant corrections were observed for organs such as the contralateral breast, yielding 0.81 vs. 0.92 DICE when corrected, compared to the GS-C. No statistically significant differences were observed for 87.5% of the absorbed dose-distribution profiles, despite some clinically relevant drawbacks (i.e. medial breast edge). A mean 475 (± 70) seconds for breast GS-C, 353 (± 25) seconds for AI and 152 (± 40) seconds for AI-C were required for delineating the breast structure sets. For the pelvic structures, a mean 752 (± 80) seconds, 201 (± 18) seconds and 367 (± 91) were observed, respectively. Differences between 51% to 68% less man-hours were found between GS-C and AI-C, favoring the latter.
Fig 1. Man hour differences between manual contours and AI with corrections in both thoracic and pelvic structures 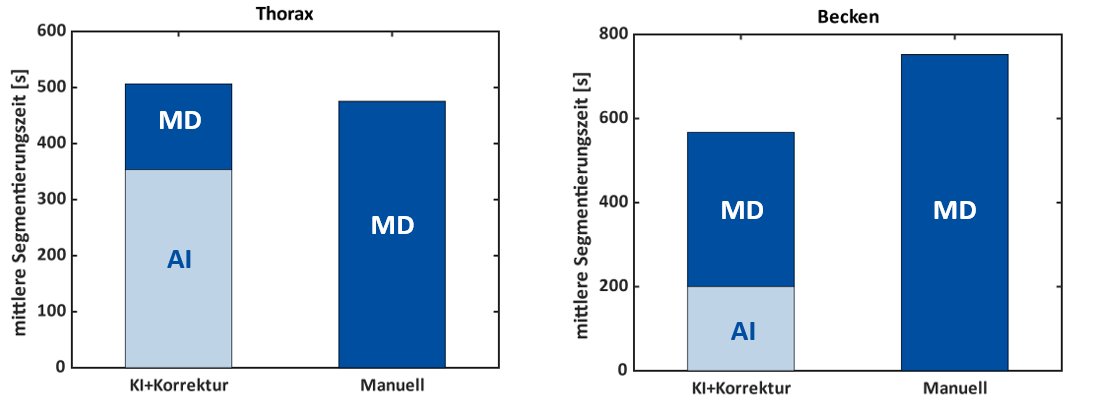
Conclusion
AI in addition to manual corrections seem to be a both safe and practical approach, granting high precision in contouring and plan applicability, while easing man power redistribution at radiotherapy services.