Physician-specific preferences yield minor differences in knowledge-based planning generated plans
PO-1638
Abstract
Physician-specific preferences yield minor differences in knowledge-based planning generated plans
Authors: Robert Kaderka1, Nesrin Dogan1, Elizabeth Bossart1
1University of Miami, Radiation Oncology, Miami, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Knowledge-based planning (KBP) models can automate, standardize and improve treatment planning. Training KBP models requires many plans, and the effect of a particular physician’s preferences on a model is unclear. We developed four head-and-neck (HN) KBP models to evaluate whether model or using a model with plans from a single physician impacts plan quality.
Material and Methods
Four HN models were built in a commercial KBP solution: “Full” was trained with 207 plans, while “Half”, Physician “A”, and Physician “B” models were trained with 101 patients each. Full and Half were trained with a mix of patients treated by physicians A and B, while the A and B model were trained with only a single physician’s plans.
As optimization objectives and priorities have a considerable impact on KBP plan quality, optimization parameters were adjusted iteratively on the Full model to maximize plan quality then applied to all models. Differences between plans created from different models result solely from variations in the training sets and not from mismatched parameters.
39 validation patients were re-planned with each of the four KBP models. Plan quality was tested in terms of dosimetric parameters for Body, PTV High/Int/Low, brainstem, cochlea, constrictors, cord, eyes, mandible, larynx, optic chiasm, optic nerves, oral cavity, parotids and submandibular glands. Each plan was compared to the manually created clinical treatment plan and the four KBP model created plans. Differences between plans were tested for significance using a paired t-test (p<0.05).
Results
The comparison of the clinical, Full and Half plans is shown in Fig. 1. The boxplot compares the distribution of mean doses with brackets indicating statistical significance. Both the Full and Half models decrease dose to the cochlea, constrictors and larynx, but increase dose to the left parotid slightly compared to the clinical plan. Dose to the left cochlea is slightly elevated and larynx dose is slightly reduced in the Half model compared to the Full model. No other parameters were statistically significant. Differences in plans between models were <0.5Gy.
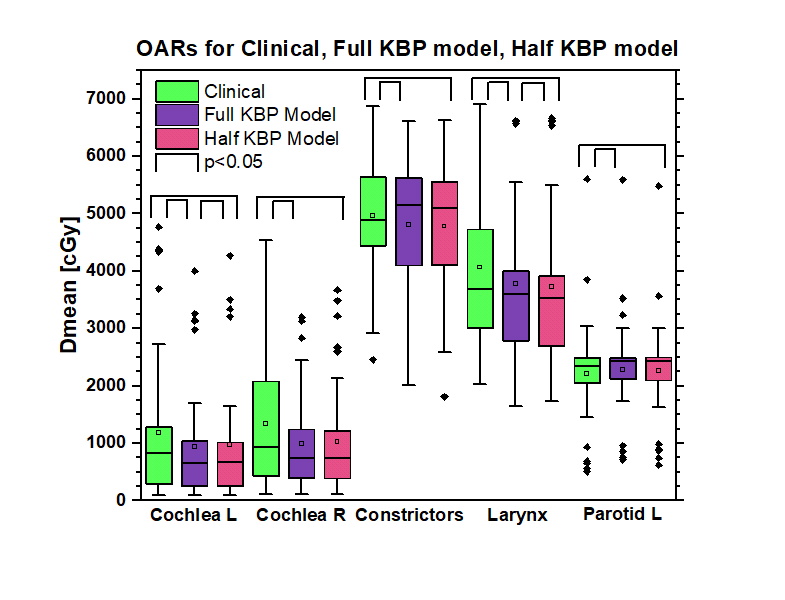
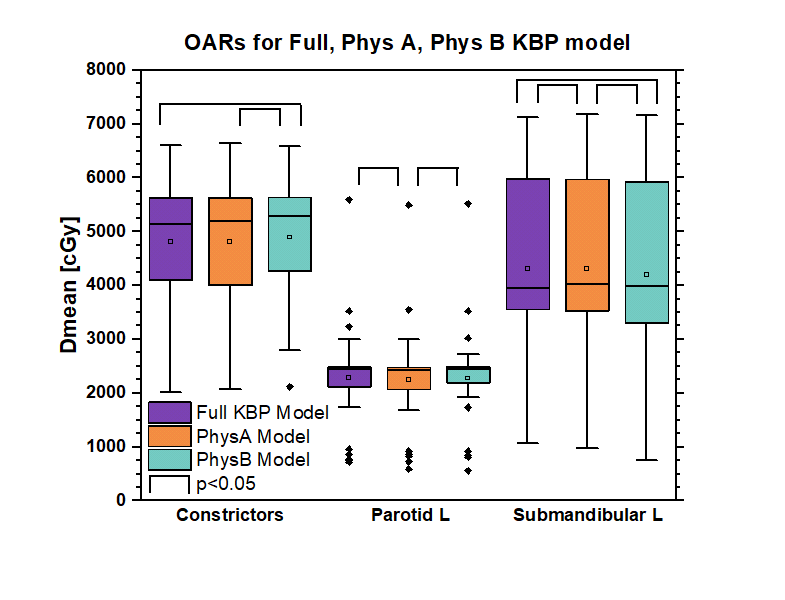
Fig. 2 compares the Full, A and B models. The only statistically significant differences between A and B plans were the constrictors, left parotid and left submandibular, with a maximum difference of 1.11Gy.
Conclusion
The four KBP models created largely equivalent plans with only a handful of significant differences of 1.11Gy or less. We did not see a substantial benefit from doubling the training of the KBP model, however, the “small” training sets of 101 plans represent a relatively large training set. Furthermore, planning preferences by planners or physicians in a KBP training set only lead to minimal differences in resulting plans. These findings indicate that it is prudent to train a general KBP model for a disease site rather than creating a multitude of models with physician specific planning preferences.