Automated clinical-criteria-driven optimal planning: clinical experience with over 6000 patients
PO-1666
Abstract
Automated clinical-criteria-driven optimal planning: clinical experience with over 6000 patients
Authors: Linda Hong1, Ying Zhou1, Qijie Huang1, Gourav Jhanwar1, Jie Yang1, Hai Pham1, Laura Cervino1, Joseph Deasy1, Masoud Zarepisheh1
1Memorial Sloan Kettering Cancer Center, Medical Physics, New York, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
To present our experience with an automated approach to IMRT treatment planning using expedited constrained hierarchical optimization (ECHO) for various disease sites including paraspinal/metastatic tumor, prostate and non-small cell lung cancer.
Material and Methods
After contouring, a template using multiple IMRT fields was created and sent to ECHO through the treatment planning system (TPS) application program interface (API) plug-in. ECHO does not use the TPS optimization engine, however, it utilizes TPS leaf sequencing and dose calculation. Institutional clinical criteria, including maximum and mean doses plus dose volume metrics, were directly employed as template ECHO input parameters to derive appropriate objective functions and constraints. ECHO applies advanced optimization tools (such as hierarchical constrained optimization, convex approximations and Lagrangian methods) to produce Pareto optimal plans. The optimal fluence map generated by ECHO was imported automatically into TPS for leaf sequencing and final dose calculation. Upon ECHO completion, the planner received an email indicating the plan was ready for review. The plan was accepted by the planner if all clinical criteria were met, otherwise a limited number of parameters could be adjusted prior to another run with ECHO.
Results
For each disease site, a template based on the established clinical criteria (limit and guidelines) was created and ECHO only required limited representative training patient data to fine tune few optimization parameters (e.g., dose fall-off criteria, slip factors). After training, the same parameters were then used to validation study of slightly more plans with a few prescription schemes and corresponding clinical criteria and compared with manual plans. Those parameter templates were then clinically implemented to plan that disease site with widely different prescription scheme and can easily adapt to changing clinical practice. If the clinical prescription schemes or criteria are modified moderately, ECHO can easily adjust to those clinical changes.
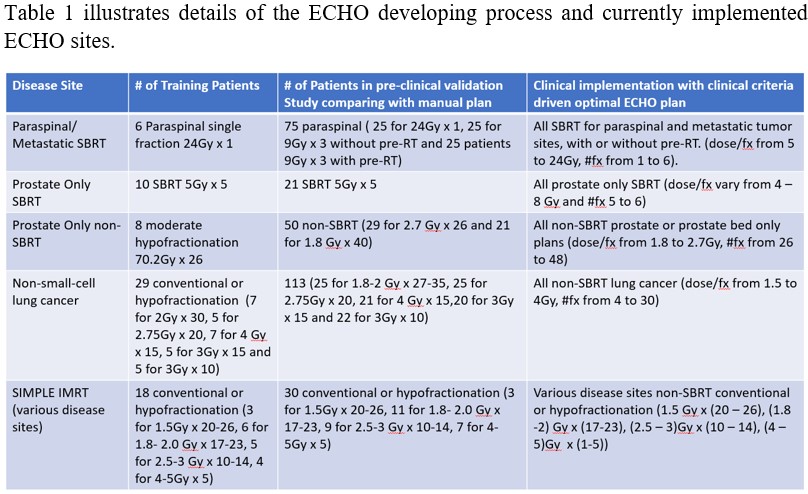
From 4/2017 to 10/2022, over 6000 patients underwent radiotherapy using 6764 ECHO produced plans. Figure 1 shows treated ECHO plans for different disease sites. PTV s varied greatly with median 91 cc (range 1.0 - 1854). The median time to produce one ECHO plan was 27 minutes (range 7 - 201) mainly depending on the PTV and patient size.
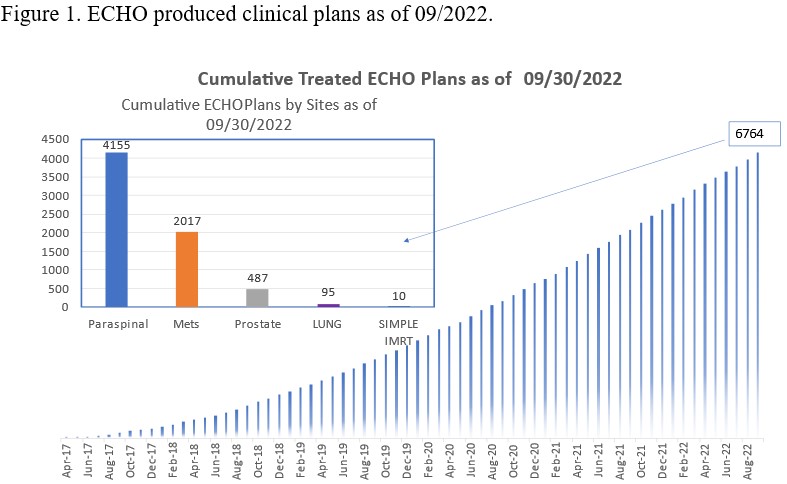
Table 2 summarize the performance of ECHO for each disease site.
| Disease Site | Only one Run (%) | Had 2 Runs (%) | Had > 2 Runs (%) | #1 rerun reason | #2 rerun reason |
| Paraspinal | 63 | 17 | 20 | some criteria not met | beam modified
|
| Oligomets | 80 | 12 | 8 | beam modified | criteria changed |
| Prostate | 88 | 5 | 7 | some criteria not met
| contour modified |
| Lung | 61 | 20 | 19 | beam modified
| criteria changed |
Conclusion
An automated treatment planning system has been clinically deployed in our institution for radiotherapy for various disease sites. ECHO saves resources and improved consistency of plan quality and enabled expedited treatment including same day SBRT treatment in our clinic.