Are ultra-hypofractionated prostate treatments worse in some patients? - an in-silico study
Fiere Claassen-Janssen,
The Netherlands
PD-0984
Abstract
Are ultra-hypofractionated prostate treatments worse in some patients? - an in-silico study
Authors: Fiere Claassen1, Veronique Coen1, Inge Jacobs1, Tom Harthoorn1, Isabelle De Marco1, Boudien Mous-Van der Wegen1, Frank Van den Heuvel1
1Zuidwest Radiotherapeutisch Instituut, Radiotherapy, Vlissingen, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
The current trend within radiotherapy is towards more hypo-fractionated (HF) treatments. In our institute, ultra-hypofractionation (UHF) treatment for prostate patients is recently introduced into the clinic.
In the initial treatment plan, dose at organs at risk is always minimized. However in practice, due to setup uncertainties and anatomical changes, the delivered dose at the organs at risk can be higher than initially planned. In UHF treatments, this effect can be more pronounced.
This study investigates the radiobiological impact, on target and organs at risk, of random and systematic errors in ultra-hypofractionated (UHF) prostate treatments compared to hypo-fractioned (HF) prostate treatments.
Material and Methods
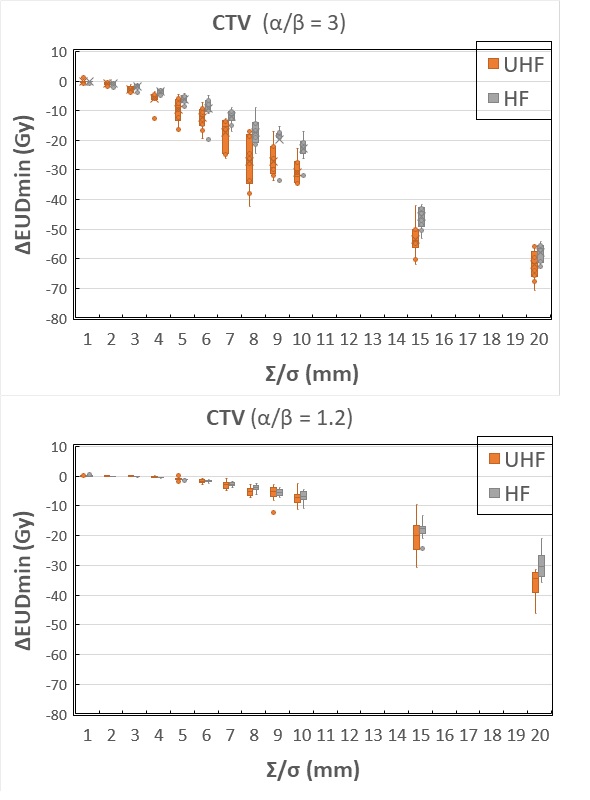
Ten patients treated for prostate cancer were selected. Treatment plans are generated for HF (20 x 3.0 Gy) and UHF (5 x 7.25 Gy). An isotropic CTV-PTV margin of 5mm is clinically used. For every patient, 20 systematic errors are generated and dose is recalculated. The random error is sampled by the number of fractions The EUD was calculated for prostate (α/β = 1.2 en α/β = 3.0), rectum (α/β = 3.0) and bladder (α/β = 3.0 and α/β = 2.0). These EUD calculations are performed for every instance (i.e. both fractionation schedules and several error scenarios). For the OARs, the difference (ΔEUDmax) between maximum EUD (Gy) and nominal EUD (Gy) is reported. For the CTV, the difference (ΔEUDmin) between minimum EUD (Gy) and nominal EUD (Gy) is reported. The ΔEUD (Gy) is plotted as a box and whisker plot as a function of the systematic (Σ) and random error (σ), shown for 10 patients. Differences between the mean ΔEUD of both arms are tested with a paired t-test.
Results
CTV coverage
Figure 1 shows ΔEUDmin for the CTV (i.e. prostate). When using α/β = 3, the minimum EUD in the CTV decreases more rapidly with setup error in the UHF arm, compared to the HF arm. The difference in mean ΔEUD between the arms is significant (p = 0.0006 and 0.0010, for α/β = 1.2 and α/β = 3 respectively). Although the difference between the groups is significant, the decrease in minimal EUD is small in the α/β = 1.2 scenario.
Organs at Risk
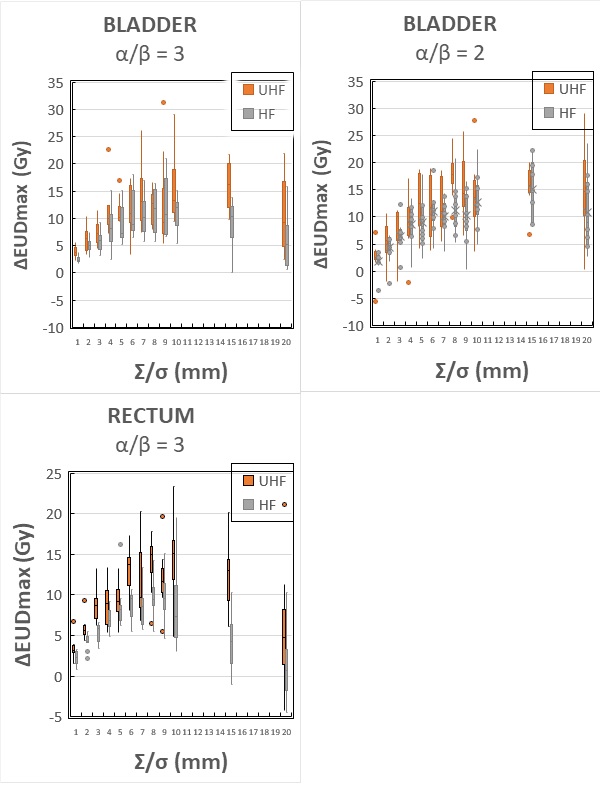
In Figure 2 the ΔEUDmax is calculated for rectum (α/β = 3) and bladder (α/β = 2 and α/β = 3). In the UHF arm, the maximum ΔEUD for the rectum increases more rapidly than in de HF arm, with increasing setup error. The difference in mean ΔEUD between the arms is significant for rectum (p = 0.0002) and bladder (p=0.001 for both α/β ratio’s).
Conclusion
In UHF, the delivered dose is more sensitive for systematic and random errors than in HF treatments. This can result in ‘unlucky patients’ with larger maximum dose on the OARs. The lower dose on the CTV due to UHF, will have less impact because of the favorable α/β ratio of the prostate. The “unlucky patients” with higher OAR dose due to UHF might benefit from a more robust planning strategy.