External validation of automated adaptive planning for EMBRACE II cervical cancer brachytherapy
OC-0130
Abstract
External validation of automated adaptive planning for EMBRACE II cervical cancer brachytherapy
Authors: Linda Rossi1, Supriya Chopra2, Rik Bijman1, Prachi Mittal3, Subhajit Panda3, Sebastiaan Breedveld1, Remi Nout4, Ben Heijmen1
1Erasmus MC Cancer Institute, Department of Radiotherapy, Rotterdam, The Netherlands; 2Advanced Centre for Treatment Research and Education in Cancer, Tata Memorial Centre. Homi Bhabha National Institite, Department of Radiation Oncology, Navi Mumbai, Maharashtra, India; 3Advanced Centre for Treatment Research and Education in Cancer, Tata Memorial Centre. Homi Bhabha National Institute, Department of Radiation Oncology, Navi Mumbai, Maharashtra, India; 4Erasmus MC Cancer Institute, Department of Radiotherapy, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
A fully-automated multi-criteria treatment planning workflow for EMBRACE II adaptive HDR brachytherapy (BT) for locally advanced cervical cancer was previously developed and tested in a single European center. Internal validation showed improved OAR doses, comparable target doses and comparable loading patterns (i.e. controlled dwell times without unacceptable hot spots or gradients and with balanced use of intracavitary (tandem), ovoids and interstitial needles). Without any modifications, the workflow was externally validated in an Indian center.
Material and Methods
Twenty patients, previously treated with 4 BT fractions of 7 Gy following image guided adaptive BT recommendations for cervix cancer, were included in the study. For each BT fraction, autoplanning aims were automatically established based on the EBRT dose and on previous auto BT fractions, aiming to achieve the clinical CTVHR D90% for plan comparison. The workflow was fully automated, without manual interference and fine-tuning of the final plans, and without any tuning for the new center.
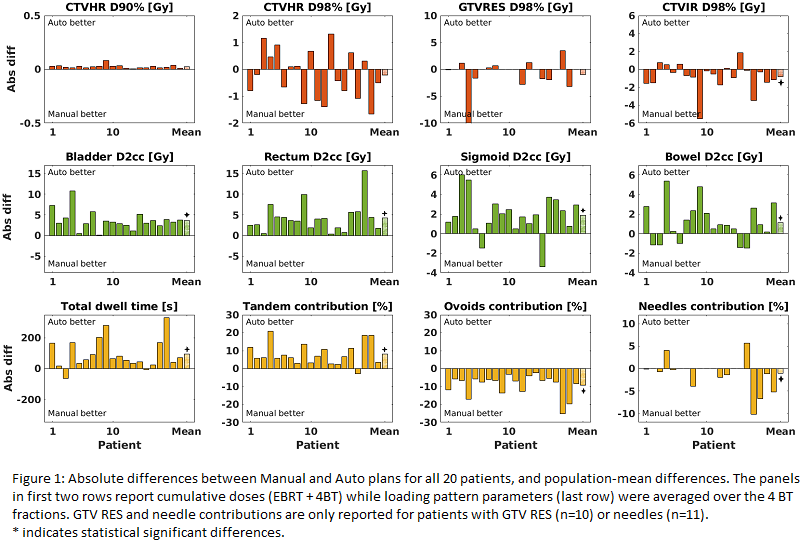
In total 80 automated plans were generated and evaluated by treating clinician. Three types of evaluations were performed to compare automatically generated plans (Auto) with clinical plans (Manual): I) dosimetrical evaluations for targets and OARs for the 20 cumulative plans (EBRT + 4BT) in total EQD2Gy, II) loading pattern evaluations, including tandem, ovoids and needle usage (contribution) as well as total dwell time for all 80 plans, III) preference by the treating clinician for all 80 fraction plans as “Auto better, Manual better or Equal”.
Results
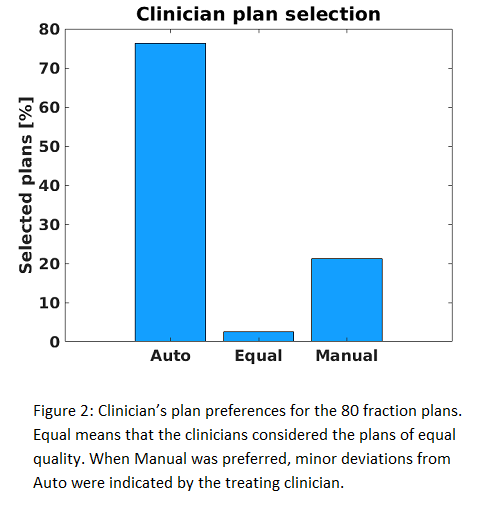
Comparable EQD2Gy target coverage was achieved for CTV HR and GTV RES (all p>0.05, figure 1), while for CTV IR D98% a difference of 0.8 Gy (p=0.02) in favour of Manual plan was found. All mean cumulative OAR doses were significantly lower with Auto: 3.6, 4.3, 1.9 and 1.1 Gy for bladder, rectum, sigmoid and bowel D2cc, respectively (all p<0.04). For bladder and rectum D2cc, all 20 patients benefitted from Auto (Fig 1). Total dwell time was reduced with Auto by 93.1 s (p<0.001). As desired, tandem contributions increased (relative increase 8.1%, p<0.001) and needle contributions decreased (2.6%, p=0.03) with Auto. Ovoids contributions were favourable for Manual (increase by 9.2% p<0.001). Clinician preferred Auto for 76.25% of fractions (61/80), Manual for 21.25% and plans were equal for 2.5% (Fig 2). When Manual was preferred, minor deviations from Auto were indicated in clinician plan scoring.
Conclusion
External validation of a fully-automated workflow for adaptive multi-criteria planning for EMBRACE II cervical cancer HDR-BT - without any workflow adjustments or manual tuning of Autoplans - showed overall superior quality of Auto compared to Manual for dosimetry, loading pattern and clinician’s preference.