HYPOCx-iRex (TCTR20210812003) a phase II RCT: 44Gy/20F VS 45Gy/25F CCRT in Cervical Cancer
Tissana Prasartseree,
Thailand
OC-0604
Abstract
HYPOCx-iRex (TCTR20210812003) a phase II RCT: 44Gy/20F VS 45Gy/25F CCRT in Cervical Cancer
Authors: Tissana Prasartseree1, Pittaya Dankulchai1, Wiwatchai Sittiwong1
1Faculty of Medicine, Siriraj Hospital, Mahidol University, Department of Radiology, Division of Radiation Oncology, Bangkok, Thailand
Show Affiliations
Hide Affiliations
Purpose or Objective
HYPOCx-iRex trial (TCTR20210812003), a phase II RCT comparing modest hypofractionated (HYPO 44Gy/20F) to conventional fractionation (CVRT 45Gy/25F) definitive concurrent chemoradiotherapy in patient with locally advanced cervical cancer, was lauched since September 2021. A pre-specified interim analysis of acute toxicity and early response rate was performed.
Material and Methods
Patients with locally advanced cervical carcinoma were enrolled, excluding patient with >=3 positive pelvic LN or pathologic LN at/above common iliac region to limit the upper border of RT field for the safety screening purpose.
External radiation dose was randomized to HYPO for 44 Gy (2.2Gy/F) to whole pelvis and 53 Gy (2.65 Gy/F) SIB at gross pelvic LN all in 20 five-day-a-week fractions, and for CVRT 45 Gy and 55 Gy (2.2Gy/F) in 25 fractions, respectively with VMAT concurrent with 40mg/m2 weekly cisplatin
Brachytherapy planning was also randomized for conventional D2cc planning or with additional iRex parameter (DOI: 10.5114/jcb.2020.100377, not in the scope of this abstract). IGABT was performed in 4-5 once to twice weekly fractions with at least one MRI planning per GEC-ESTRO recommendation.
Overall treatment time was restricted to 42 days for HYPO and 49 days for CVRT.
With a target of 40 patients, an interim analysis at 3-mo follow up time of the first 20 patients was pre-specified for toxicity evaluation with CTCAEv5, tumor response, and Quality of life (QOL) with QLQ-C30, EN24 and Cx24.
Results
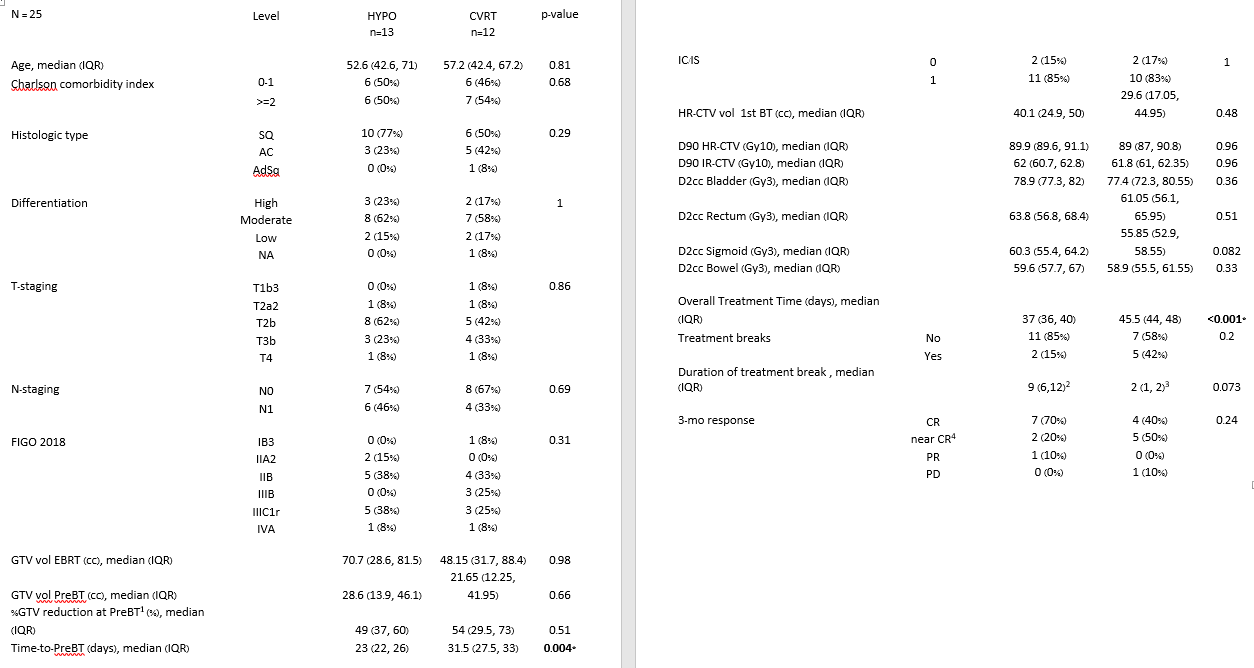
25 patients were included the report with characteristics shown in Table 1.
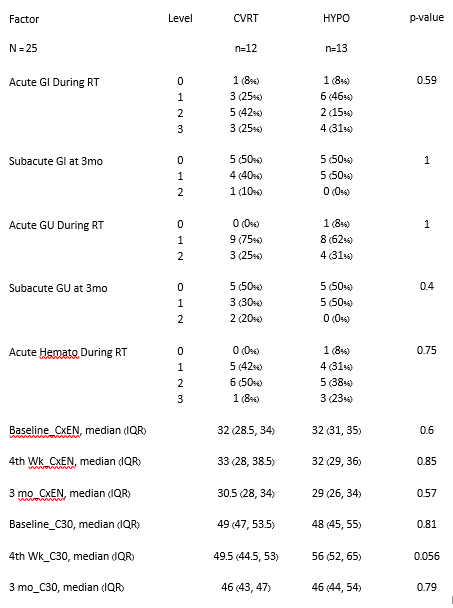
13 patients in HYPO and 12 patients in CVRT received non-significant difference of HR-CTV and IR-CTV D90, and bladder, rectum, sigmoid and bowel D2cc (Table1). OTT was significantly lower in HYPO with median of 37 days comparing to 45 days in CVRT. No significant difference in terms of toxicity were observed. Specifically acute ≥Grade 3 gastrointestinal (GI), genitourinary (GU), hematology were seen in HYPO and CVRT with 3(25%) and 4(31%), 0 and 0, 1(8%) and 3(23%), respectively. These toxicities were subsided within 3 months as shown in Table2. No significant in difference of %GTV reduction at the time of pre-brachytherapy evaluation, despite shorter time-to-brachytherapy in HYPO. Higher rate of CR was observed in HYPO, however without statistical significance (Table1). In terms of QOL, no significant difference were observed.
Conclusion
Moderately hypo-fractionated RT 44Gy/20F with concurrent cisplatin showed no significant difference in acute toxicity and tumor response comparing to 45Gy/25F in this interim analysis. Significantly reduced OTT were achieved, moreover maintain ability to reduce GTV before brachytherapy. Longterm result after completion of HYPOCx-iRex is awaited to elucidate the non-inferiority of hypofractionated RT in locally advanced cervical cancer.