Geometric stability during Stereotactic Arrhythmia Radiotherapy
OC-0942
Abstract
Geometric stability during Stereotactic Arrhythmia Radiotherapy
Authors: Rianne de Jong1, Niek van Wieringen1, Martijn van Ree2, Edith Dieleman1, Pieter G. Postema2, Jorrit Visser3, Brian Balgobind1
1Amsterdam UMC, Radiation Oncology, Amsterdam, The Netherlands; 2Amsterdam UMC, Cardiology, Amsterdam, The Netherlands; 3Amsterdam, Radiation Oncology, Amsterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Patients with therapy-refractory ventricular tachycardia were enrolled in the STARNL-1 trial to receive non-invasive stereotactic arrhythmia radiotherapy with a single high dose fraction. As these patients are in a poor condition, target volumes may show excessive instability. Hence, we retrospectively quantified the geometric stability of the target volumes to assess our imaging and correction strategies.
Material and Methods
Between December 2020 and October 2021 7 patients were enrolled, 6 in STARNL-1 trial, 1 compassionate use. The Internal target volume (ITV) was defined as the pro-arrhythmic ventricular region with correction for breathing motion using a 4DCT-scan. All patients were male. PTV margin around the ITV was 5 mm. PTV volumes were on average 216 cm3 (range 93-300 cm3). A single fraction dose of 25 Gy was prescribed to the PTV. For all patients a 10 MV FFF 3 arc VMAT plan was designed. Image guidance was performed using online CBCT, matching on the target volume, correcting translational errors only. A correction is always evaluated using a verification CBCT scan with a 3 mm action level in vector length for the residual error. As this procedure resulted in a total of 7 CBCT scans for patient 1, the IGRT procedure was expanded to an online No Action Level (NAL) imaging procedure (4 CBCT scans pretreatment) for patient 2 to 7 (3 times CBCT scan calculating average displacement, followed by a table correction). Additionally, a practice run with only CBCT imaging was introduced 1 day before treatment assuring patient compliance and adequate treatment delivery with respect to stability of the patient and target volume. For all patients a post treatment CBCT scan was acquired. This resulted in a total of 67 CBCT scans for analysis. The CBCT match results are corrected for table shifts executed after previous CBCT scans. To report the stability of the target the standard deviation (SD) of the processed match results for all fractions was calculated. On-table times were all below 50 minutes. Beam-on times were on average 276 seconds with a maximum of 313 seconds.
Results
For patient 1 a total of 6 pre- and mid-treatment CBCT scans were needed to concur with the 3 mm vector length residual motion threshold before start of treatment and in between arcs . For patient 2-7 for all fractions the residual vector length was below the set threshold of 3 mm. The mean standard deviation was 0.11 cm (LR), 0.19 cm (CC), 0.12 cm (AP). The range of standard deviations was 0.03–0.35 cm (LR), 0.03–0.39 cm (CC), 0.04–0.28 cm(AP). Figure 1 shows results per patient.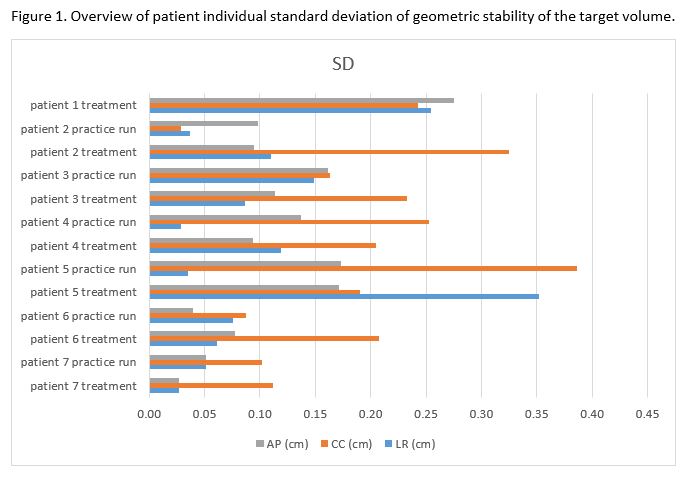
Conclusion
In this cohort of patients treated with stereotactic arrhythmia radiotherapy, patient 1 had a large intra fraction motion exceeding the action level of 3 mm residual set up error vector length after single CBCT match evaluation. This prompted an online NAL imaging procedure for patient 2 to 7. To avoid problems with treatment delivery the online NAL imaging procedure will be continued for future patients in the STARNL-2 trial.