Assessment of cardiorespiratory motion for cardiac radioablation using a digital 17-segment model
Raoul R.F. Stevens,
The Netherlands
OC-0940
Abstract
Assessment of cardiorespiratory motion for cardiac radioablation using a digital 17-segment model
Authors: Raoul Stevens1, Colien Hazelaar1, Marta Bogowicz1, Rachel M.A. ter Bekke2, Paul G.A. Volders2, Karolien Verhoeven1, Dirk de Ruysscher1, Joost J.C. Verhoeff3, Martin F. Fast3, Stefano Mandija3, Jakub Cvek4, Lukas Knybel4, Pavel Dvorak4, Oliver Blanck5, Wouter van Elmpt1
1GROW - School for Oncology, Maastricht University Medical Center+, Radiation Oncology (Maastro), Maastricht, The Netherlands; 2CARIM - School for Cardiovascular Disease, Maastricht University Medical Center+, Cardiology, Maastricht, The Netherlands; 3University Medical Center Utrecht, Radiotherapy, Utrecht, The Netherlands; 4University Hospital and Faculty of Medicine, Oncology, Ostrava, Czech Republic; 5University Medical Center Schleswig-Holstein, Radiation Oncology, Kiel, Germany
Show Affiliations
Hide Affiliations
Purpose or Objective
The impact of various motion management strategies, such as the internal target volume (ITV) approach or treatment in breath-hold, for stereotactic arrhythmia radioablation (STAR) is not fully understood. We developed a comprehensive framework using a digital CT phantom that allows simulation of cardiorespiratory motion in combination with different motion management strategies to gain more insight in the impact of cardiorespiratory motion on STAR.
Material and Methods
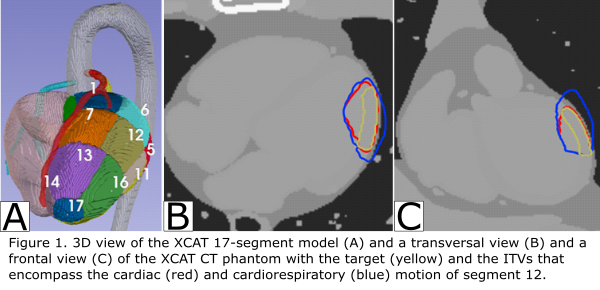
The 4D extended cardio-torso XCAT CT phantom (Segars, 2010) was expanded with the 17-segment heart model, a standard in cardiology used to describe left ventricle (LV) anatomy. Segments were parametrized in XCAT to create heart lesions based on the anatomical region definitions from the 17-segment model. This allowed placement of targets within the phantom based on these standardized heart regions. Next, we simulated cardiac (5 phases) and respiratory-gated (10 phases) 4D-CTs applying cardiorespiratory motion during free-breathing and breath-hold (cardiac motion only). Translation of the heart due to breathing was set to population-averaged values measured in VT patients, i.e. 14, 8, and 0mm in the Sup-Inf, Ant-Pos, and Left-Right direction, respectively. Cardiac contraction was set to baseline XCAT values. Next, the targets were extracted from all phases and used to construct ITVs that encompass the complete cardiac and/or respiratory target motion to quantify cardiorespiratory motion (Figure 1). In addition, we investigated the clinical imaging scenario when cardiac motion is not fully captured during a 4D respiratory CT scan for radiotherapy planning. Hereto, ITVs that included only specific cardiac phases (diastolic or diastolic and systolic) in combination with all respiratory phases were created. Geometric coverage (overlap of the ITV with the cardiorespiratory ITV) was calculated to evaluate these ITVs.
Results
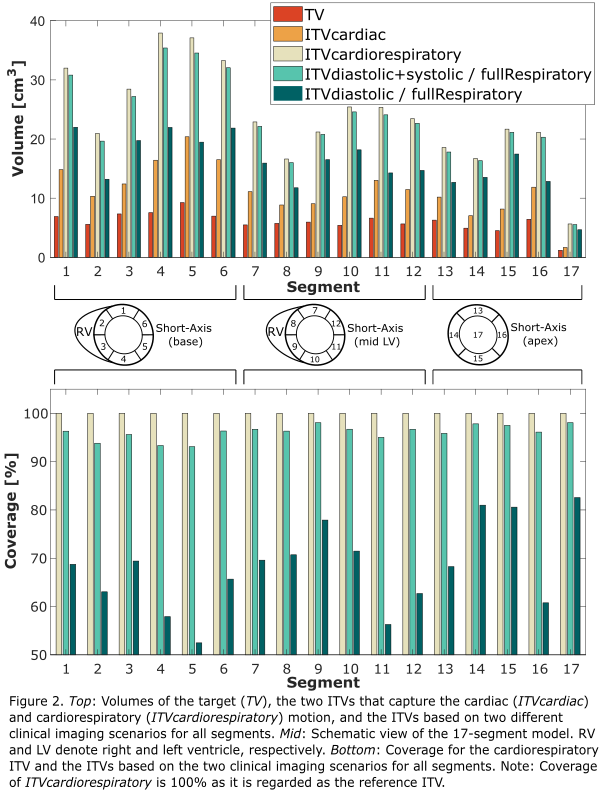
Volumes of the 17 segments were on average 6cm³ [1-9cm³] (see Figure 2). Full cardiac motion resulted in an ITV that was 83% larger than the corresponding segment volumes (ITV: 11cm³ [2-20cm³]), whereas the ITV increased by 300% compared to the segment volumes (ITV: 24cm³ [5-38cm³]) because of both cardiac and respiratory motion.
The ITV incorporating only the diastolic phase and all respiratory phases had a mean coverage of 68% [52-83%] which was almost 40% smaller than the coverage of the ITV that also included the systolic cardiac phase, i.e. 96% [93-98%]. ITVs for segments located towards the free wall of the LV showed lower coverage compared to segments on the septal side.
Conclusion
A framework was developed that allows assessment of motion in combination with different motion management strategies for STAR. Our results indicate that careful assessment of patient-specific motion is needed to create representative ITVs. In future research, our framework can also be used to analyze radiotherapy dose distributions for different treatment and motion management strategies to perform a full dosimetric analysis.