NTCP reduction in head-and-neck cancer VMAT using robust planning
Marcel van Schie,
The Netherlands
OC-0451
Abstract
NTCP reduction in head-and-neck cancer VMAT using robust planning
Authors: Marcel van Schie1, Anna Petoukhova1, Linda Rossi2, Lienke Kwakkel-Huizenga3, Stefan Hutschemaekers3, Ben Heijmen2
1Haaglanden Medical Center, Medical Physics, Leidschendam, The Netherlands; 2Erasmus MC Cancer Institute, Radiation Oncology, Rotterdam, The Netherlands; 3Haaglanden Medical Center, Radiation Oncology, Leidschendam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Radiotherapy treatment planning of head-and-neck cancer is challenging for its anatomical complexity, numerous surrounding OARs and multiple dose levels involved. In robust planning, the CTV dose is directly optimized, omitting the use of a PTV. We investigated the potential of scenario-based robust VMAT planning in head-and-neck cancer to improve target coverage and reduce NTCPs for xerostomia and dysphagia.
Material and Methods
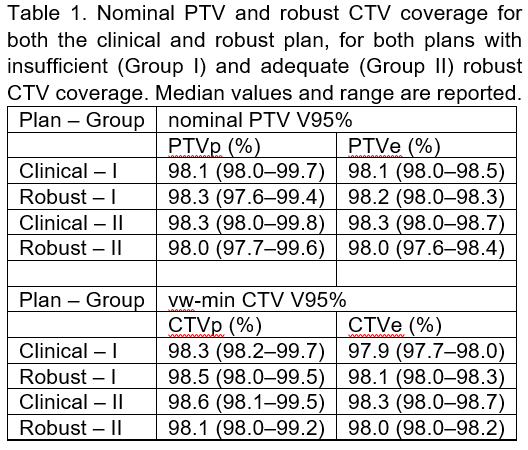
Eighteen pharyngeal head-and-neck cancer patients were included. Planning was performed with RayStation version 9B and delivered in 2021. For each patient, the clinical PTV-based SIB VMAT plan was first robustly evaluated for CTV coverage, using 14 setup error scenarios with a 3 mm translation, corresponding to the applied PTV margin. This evaluation focussed on the voxel wise minimum (vw min) CTV dose [1]. Analogous to the clinical PTVs, primary CTVp and elective CTVe were cropped to 5 mm from the body contour, to avoid dose calculation in the dose build up region. CTV coverage was considered acceptable if V95% ≥ 98% in the vw-min distribution (robust CTV coverage). Next, two patient groups were identified based on the robust CTV coverage of the clinical plans.
Group I (5 patients): for clinical plans with insufficient robust coverage of either of the CTVs, a robust min dose objective was added for the corresponding CTV and robust optimization with 6 scenarios was performed, aiming to achieve minimal robust CTV coverage and reduce OAR doses. Group II (13 patients): for clinical plans with adequate robust CTV coverage, first further optimization was performed to reduce OAR doses. Next, as for Group I, a robust min dose objective was added when robust CTV coverage was getting compromised.
Plans were compared based on PTV coverage and robust CTV coverage. Moreover, using OAR mean doses, NTCP values were evaluated for the risk of dysphagia and xerostomia [2].
Results
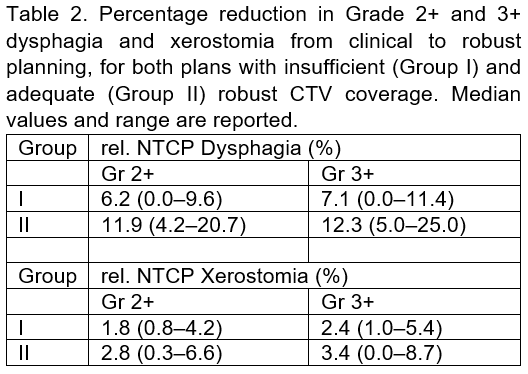
Results: In Group I, robust optimization resulted in improved robust CTV coverage in all plans (see table 1). In Group II, PTV coverage was omitted in favour of sparing OARs. Robust CTVe coverage was slightly reduced but kept above 98% in all plans. Reductions in NTCP due to robust planning are shown in Table 2. In both patient groups, all patients had reduced NTCPs for both dysphagia and xerostomia. Reductions were largest for dysphagia in Group II, with median reductions of 11.9% for Gr 2+ and 12.3% for Gr 3+.
Conclusion
Conclusion: We proposed a new approach for incorporating robust planning in clinical VMAT plan generation for head-and-neck cancer. While obtaining clinically acceptable plans with robustness in CTV coverage, robust plans also had clinically relevant NTCP reductions, especially for dysphagia.
References:
[1] Korevaar E.W. et al. Radiother Oncol. 2019;141:267–274.
[2] Langendijk J.A. et al. Int J Part Ther. 2021;8(1):354–365.