ESTRO-Elekta Brachytherapy Award: MRI-guided robotic needle insertion for prostate brachytherapy: proof of principle patient study
Marinus Moerland,
The Netherlands
OC-0295
Abstract
MRI-guided robotic needle insertion for prostate brachytherapy: proof of principle patient study
Authors: Marinus Moerland1, A.L.H.M.W. van Lier1, L.J. van Schelven2, M.J.A. Rasing3, M. Peters1, E. Boskovic2, R.I. Schokker3, K.M. van Vliet-van den Ende3, D.D. Kelder3, J. Verkerk3, S.M.G. van de Pol3, J.J.W. Lagendijk3, J.R.N. van der Voort van Zyp1
1University Medical Center Utrecht, Radiation Oncology, Utrecht, The Netherlands; 2University Medical Center Utrecht, Medical Technology & Clinical Physics, Utrecht, The Netherlands; 3University Medical Center Utrecht, Radiation Oncology , Utrecht, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
A robotic needle implant device for MR guided high dose rate (HDR) prostate brachytherapy is under development at the University Medical Center Utrecht. The purpose of this study is to test the feasibility and accuracy of inserting a BT needle into the prostate (n=5) to a defined target point using the robotic device.
Material and Methods
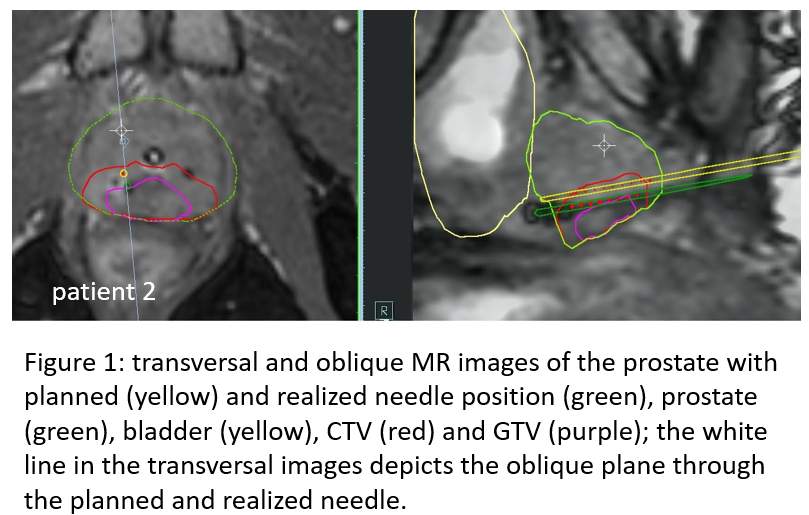
The robot fits in a 1.5 T MR scanner and is placed between the patient’s legs. While scanning, the needle is stepwise inserted using a pneumatic tapping device to reduce prostate deformation. The needle can be shifted and angulated to have access to the whole prostate. Five patients were included between November 2019 and June 2022. GTV and CTV were delineated based on diagnostic MRI and PET, and a preplan was made to assess needle configuration. At the start of a session, an MR scan was made in treatment position and fused with the diagnostic MR images. One of the preplanned needle positions was selected for robot insertion. The needle target point was determined on the MR image. The needle entry point and angles were set for the target point, and the needle was tapped towards the target point while monitored with dynamic MRI. At final depth, an MR scan was made to verify the needle position and adapt the treatment plan, after which the dose was delivered. The remaining needles were inserted manually using our regular clinical procedure. Accuracy of robotic needle insertion was analyzed by comparing the planned and the realized needle tip positions in MR coordinates. Deviations were calculated as Euclidian distance in the axial plane between planned and realized position. The deviation to the geometric target point was called needle tip geometric deviation (NTG). The deviation of the needle tip with respect to the prostate tumour target point was called needle tip tumour deviation (NTT) and was calculated by fusing the MR scans before and after needle insertion using the fusion module of the TPS. Difference between NTT and NTG is a measure for prostate movement. Duration of the robotic procedure was recorded.
Results
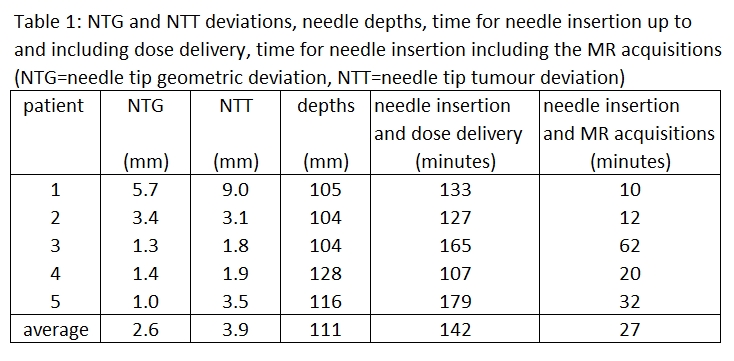
The robotic device was able to tap the needle into the prostate to the planned needle depths. The needle insertion and dose delivery (including setup robot, MR scanning, reconstruction and planning) took 142 (range 107-179) minutes, of which the needle insertion and MR acquisitions took 27 (10-62) minutes. NTG deviation amounted 2.6 (range 1.0-5.7) mm and NTT deviation amounted 3.9 (range 1.9-9.0) mm. From patient 3 onwards a slightly altered needle positioning procedure was followed, which reduced the deviations. There was no indication of bending of the needle in the 5 procedures. No additional toxicity was reported. In patient 5 the total CTV dose of 19 Gy was delivered by the robotic needle. To our knowledge, this was the first robotic MRI guided BT treatment.
Conclusion
This study shows that MRI guided robotic needle insertion is feasible with accuracy in the order of 3 to 4 mm and prostate movement in the order of 1 to 3 mm.