Fully automated robust multi-criterial treatment planning for HNC IMPT
Merle Huiskes,
The Netherlands
OC-0285
Abstract
Fully automated robust multi-criterial treatment planning for HNC IMPT
Authors: Merle Huiskes1, Wens Kong2, Eleftheria Astreinidou1, Koen Crama1,3, Sebastiaan Breedveld2, Ben Heijmen2, Coen Rasch1,3
1Leiden University Medical Centre, Radiation Oncology, Leiden, The Netherlands; 2Erasmus MC Cancer Institute, Radiotherapy, Rotterdam, The Netherlands; 3HollandPTC, Radiation Oncology, Delft, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Automated treatment planning can decrease IMRT and VMAT planning times while obtaining also high plan quality and consistency. An example of an automated treatment planning system is Erasmus-iCycle, which produces Pareto optimal dose distributions using multi-criterial optimization based on a pre-defined wish-list. Erasmus-iCycle is already implemented in clinical practice for photon therapy, with proven equal or improved plan quality compared to manual planning. Yet, for intensity modulated proton therapy (IMPT) this has to be investigated. In this study, we investigated the quality of automatically generated robust IMPT plans against manually created clinical robust IMPT plans for head and neck cancer (HNC) patients.
Material and Methods
iCycle automated planning was applied to 30 HNC patients who were previously treated with IMPT with 7000 cGy prescription dose to the primary tumor (CTV7000) and 5425 cGy dose prescription to the elective volumes (CTV5425). The iCycle wish-list was configured for automated generation of four-beam robust IMPT plans in line with clinical requirements. For robust target coverage optimization, 21 scenarios with 3 mm setup error and ±3% density uncertainty were included for the clinical target volumes (CTVs), similar to the clinical treatment plans. A comparison between the automated iCycle IMPT plans and clinical IMPT plans was performed based on OAR doses and (robust) target coverage. Robust target coverage was assessed in the voxel-wise minimum (vw-min) dose constructed from the robust scenarios, similar to evaluation in clinical practice, with D98%>95% criterion. A Wilcoxon signed rank test was performed to assess if there was a statistically significant difference (p<0.05) between the iCycle and clinical plans.
Results
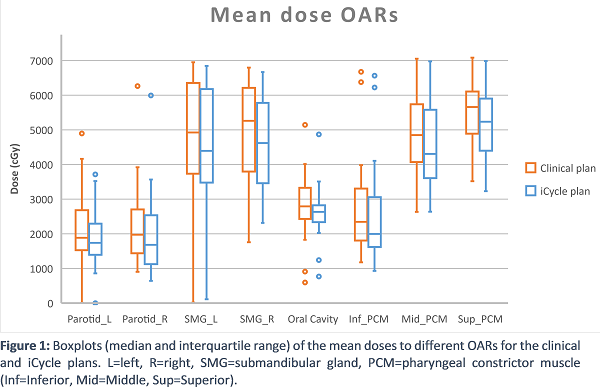
For the nominal scenario, the D98 in all clinical and iCycle plans fulfilled the D98>95% criterion for both CTVs. The D98 in the iCycle plans was on average (± SD) comparable in both CTVs compared to the clinical plans (CTV7000: 6892±14 cGy vs. 6889±25 cGy, CTV5425: 5453±29 cGy vs. 5378±19 cGy for the iCycle and clinical plans respectively). In the vw-min dose, the D98 for both CTVs fulfilled the D98>95% criterion in 29/30 iCycle plans, while in the clinical plans this criterion was fulfilled in 27/30 patients. For the vw-min dose, the D98 was on average comparable for both CTVs in the iCycle plans as compared to the clinical plans (CTV7000: 6677±14 cGy vs. 6697±40 cGy, CTV5425: 5254±19 cGy vs. 5197±28 cGy, for the iCycle and clinical plans respectively). The average mean dose to all evaluated OARs was lower in the iCycle plans compared to the clinical plans, see figure 1. This difference was statistically significant for all evaluated OARs, with p<0.05.
Conclusion
iCycle was able to automatically produce acceptable HNC IMPT plans with comparable (robust) target coverage D98 and statistically significant lower mean doses to OARs.