Practical and effective ART alternatives in H&N IMPT approaching daily in-room replanning quality
Michelle Oud,
The Netherlands
OC-0289
Abstract
Practical and effective ART alternatives in H&N IMPT approaching daily in-room replanning quality
Authors: Michelle Oud1,2, Sebastiaan Breedveld1, Marta Gíżyńska2, Steven Habraken1,2, Zoltán Perkó3, Ben Heijmen1, Mischa Hoogeman1,2
1Erasmus MC Cancer Institute, University Medical Center Rotterdam, Department of Radiotherapy, Rotterdam, The Netherlands; 2HollandPTC, Department of Medical Physics & Informatics, Delft, The Netherlands; 3Delft University of Technology, Department of Radiation Science and Technology, Delft, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
While daily online replanning (DailyPlan) may be considered the ultimate dosimetric solution to account for inter-fraction anatomical changes and patient setup errors in IMPT, issues with computation speed and online QA hinder clinical implementation. Therefore, robust planning combined with ad-hoc offline replanning (ClinAdapt) is currently used in clinical practice. The aim of this simulation study was to dosimetrically compare DailyPlan and ClinAdapt to three practical alternative ART strategies in head-and-neck (H&N) IMPT, weekly offline replanning (wOffR) and two strategies with daily plan selection from offline generated patient-specific plan libraries (PL1 & PL2).
Material and Methods
15 H&N IMPT patients with 3-6 repeat CTs (rCT) were included.
DailyPlan consisted of daily online replanning with 1mm setup robustness setting (SRS) and 3% range robustness setting (RRS). ClinAdapt consisted of an initial treatment plan generated for the planning CT (pCT) using 3 mm/3% SRS/RRS, and ad-hoc replanning based on clinical evaluation.
The investigated ART alternatives were: 1) wOffR: weekly offline replanning with 2mm/3% SRS/RRS; 2) PL1: using daily in-room imaging for plan selection from a pre-treatment generated PL (created using the pCT with 0, 1, 2, 3, or 5 mm SRS and 3% RRS for each patient); 3) PL2: a progressive library following the concept of PL1, but with the PL weekly extended with offline replans using rCTs. For PL1&2, daily online plan selection was based on target coverage recomputed on rCTs.
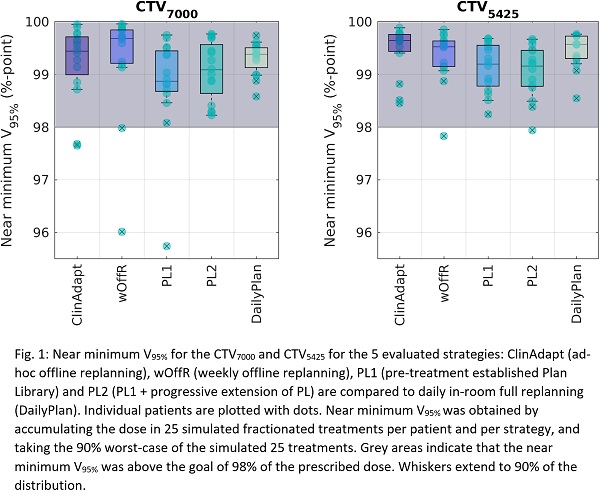
For evaluation, 25 fractionated treatment courses were simulated for each patient for all 5 strategies, using known setup and range error distributions. All strategies used propagated contours that were manually adjusted. Fraction doses were accumulated. Near-minimum target coverage and NTCPs (using Wilcoxon-signed-rank) in the simulated treatments were compared to DailyPlan.
Results
In DailyPlan, 15/15 patients had a near minimum CTV V95% above the requested 98% for both CTVs. For PL1&2 this was 14/15, compared to 13/15 for ClinAdapt and 12/15 for wOffR (Fig.1).
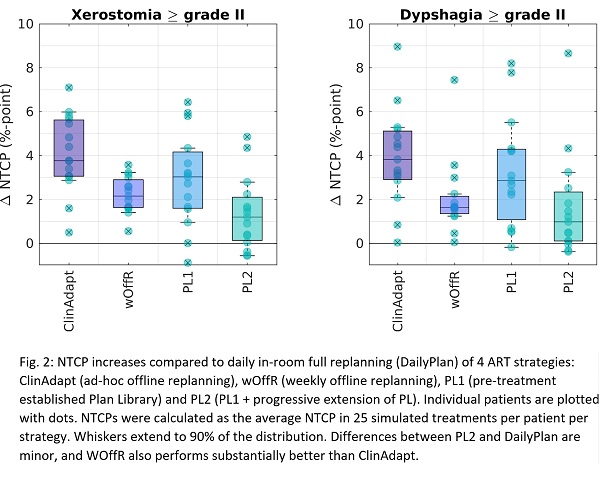
NTCP differences from DailyPlan are presented in Fig.2. Average differences between DailyPlan and ClinAdapt were 4.1±1.9%-point for xerostomia (XS) and 3.9±2.2%-point for dysphagia (DP), in favor of DailyPlan (p<0.001 for both). NTCPs of PL2 approached those of DailyPlan with differences of only 1.4.±1.7%-point for XS and 1.6±2.4%-point for DP (p<0.001 for both) in favor of DailyPlan. With PL2, 74% (XS) and 73% (DP) of the NTCP reduction could be achieved that can be realized with DailyPlan on average. For wOffR, these percentages were 40% and 43%.
Conclusion
With acceptable target coverage, NTCP reductions with the progressive plan library approach (PL2) approached those obtained with daily in-room re-planning (DailyPlan). Weekly offline re-planning (wOffR) also showed NTCP reductions compared to ClinAdapt, but to a lesser extent. Implementation of PL2 would avoid problems of DailyPlan with computation speed and online plan QA.