Results of multi-centric 4DCT QA audit: evaluating the accuracy and consistency of 4D imaging
Jinane Bakkali Tahiri,
Belgium
OC-0111
Abstract
Results of multi-centric 4DCT QA audit: evaluating the accuracy and consistency of 4D imaging
Authors: Manuela Burghelea1, Jinane Bakkali2, Martin Kyndt3, Akos Gulyban4, Jennifer Dhont1, Julliane Szkitsak5, Evelien Bogaert6, Nick Reynaert1, Dirk van Gestel7
1Institute Jules Bordet, Medical Physics, Brussels, Belgium; 2GasthuisZusters Antwerpen Ziekenhuizen, Medical Physics Department, Antwerp, Belgium; 3MIM Software Inc., Development , Brussels, Belgium; 4Institute Jules Bordet, Medical Physics , Brussels, Belgium; 5Universit¨atsklinikum Erlangen, Department of Radiation Oncology, Erlangen, Germany; 6Ghent University Hospital, Department of Radiotherapy-Oncology, Ghent, Belgium; 7Institute Jules Bordet, Radiation Oncology, Brussels, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
In this study, a multi-institutional multi-vendor 4DCT audit was initiated to assess the accuracy of current 4DCT imaging protocols.
Material and Methods
The audit consisted of a validated, comprehensive, and automatic 4DCT QA workflow; five regular and three irregular breathing patterns were applied on a 2cm sphere inside a dynamic Thorax phantom (CIRS, Norfolk, USA). 4DCT acquisitions followed the institution’s own protocol with the in-house breathing monitoring system. No manual intervention was allowed during acquisition. To comply with the automated workflow each participating institution was asked to reconstruct a static, 10-phase, MaxIP, and AvgIP image set per breathing pattern. Post-acquisition, the sphere was automatically segmented in all relevant image sets and an ITV structure was automatically created through a summation of the sphere in each phase. CT number accuracy, volume deviation, amplitude deviation, and spatial integrity were assessed per pattern using both the segmented volumes and line profiles.
Ten institutions (8 in Belgium and 2 in France) were asked to participate in the 4DCT audit and provide the image sets for analyses.
Results
Eleven institutions (three vendors, six CT scanner types, and three breathing monitoring systems) participated in the audit (7 site visits, 3 remote).
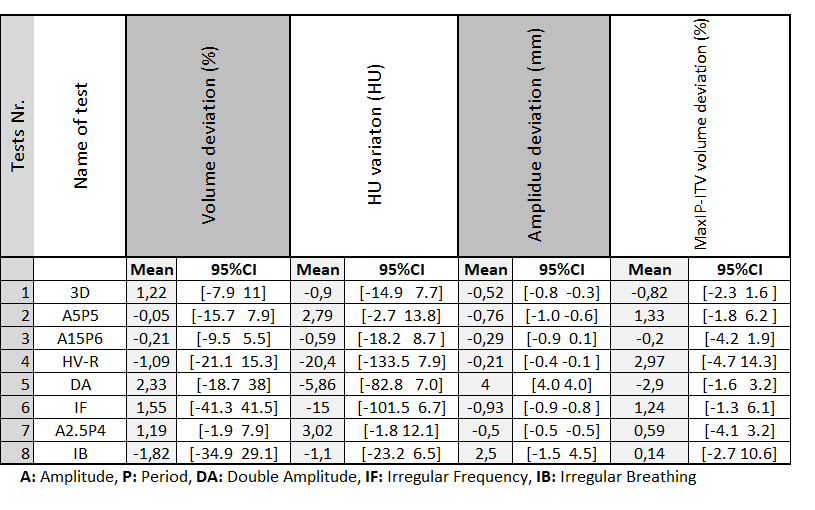
Four out of five regular breathing patterns showed relatively accurate results across all institutions (Table), with mean volume and CT number deviations below 2% and 3 HU, respectively. However, outliers in certain phases did occur. For the regular pattern with the highest velocity, substantial blurring of the sphere was observed in some phases leading to an incorrect tumor shape across all institutions (HV-R in Figure A-B).
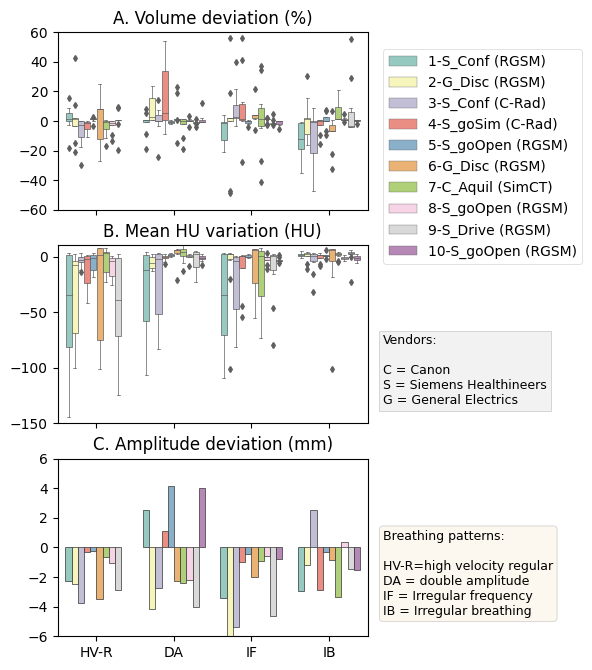
Results with all irregular patterns show more variation across the institutions (Figure A-B). Volume and HU deviations co-occurred with a blurring of the sphere, interpolation - or double-structure artifacts, which were confirmed in the line profiles.
The amplitude median deviations across the institutions were generally within 2mm for all motion directions, but larger deviations were observed for some of the irregular patterns (Figure C). MaxIP and ITV correctly captured the applied motion amplitude with deviations across all institutions within 2mm.
No obvious patterns were observed in the results related to specific institutional protocols, vendors or breathing monitoring systems.
Conclusion
Based on the high participation rate and discussions with audit participants, we observed a strong need for a comprehensive but easy-to-execute 4DCT QA workflow. The largest deviations in the results across institutions, which could have a clinically relevant impact, also confirm that a standardized multi-institutional 4DCT audit is warranted.