Gain from respiratory gating in left-sided partial breast irradiation in the DBCG PBI trial
Kristine Wiborg Høgsbjerg,
Denmark
OC-0766
Abstract
Gain from respiratory gating in left-sided partial breast irradiation in the DBCG PBI trial
Authors: Kristine Høgsbjerg1, Else Maae2, Anders Navrsted Pedersen3, Mette Møller4, Mette Holck Nielsen5, Mette Skovhus Thomsen6, Birgitte Vrou Offersen7
1Aarhus University Hospital, Department of Oncology and Department of Experimental Clinical Oncology, Aarhus, Denmark; 2Vejle Hospital, University Hospital of Southern Denmark, Department of Oncology, Vejle, Denmark; 3Copenhagen University Hospital, Rigshospitalet, Department of Oncology, Copenhagen, Denmark; 4Aalborg University Hospital, Department of Oncology, Aalborg, Denmark; 5Odense University Hospital, Department of Oncology, Odense, Denmark; 6Aarhus University Hospital, Department of Medical Physics, Aarhus, Denmark; 7Aarhus University Hospital, Department of Experimental Clinical Oncology and Department of Oncology, Aarhus, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Partial breast irradiation (PBI) has been Danish Breast Cancer Group (DBCG) standard treatment for selected breast cancer (BC) patients since 2016 based on early results from the randomised DBCG PBI trial. It is also DBCG standard to use respiratory gated radiation therapy (RGRT) in left-sided BC patients. RGRT was introduced in Danish centres during the accrual of patients in the trial. The purpose of our study is to investigate the effect of RGRT on mean heart dose (MHD) in left-sided PBI.
Material and Methods
In total, 865 patients (434 WBI, 431 PBI) were randomised in in five centres in the DBCG PBI trial from 2009-2016, and 230 patients (27%) had left-sided PBI. These patients were separated into those with upper (tumor bed plus 3 mm from papilla and cranial) versus lower located tumors (the rest). MHD and use of RGRT was registered for all patients. The MHD was not normal distributed, and the p-value was therefore calculated by Wilcoxon-Mann-Whitney-test.
Results
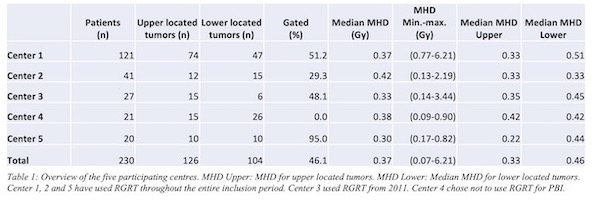
126 patients had upper located tumors, and 104 patients had lower located tumors (table 1). 66 (52.4%) of the upper located tumors received RGRT and 60 (47.6%) received free breathing radiation therapy (FBRT). Similarly, for the lower located tumors, 57 (54.8%) received RGRT and 47 (45.2%) received free breath (FBRT).
The use of RGRT varied during the period of accrual from 30.3% to 71.1% of the randomised patients and the proportion of patients received RGRT varied from 0 to 95% between the participating centres.
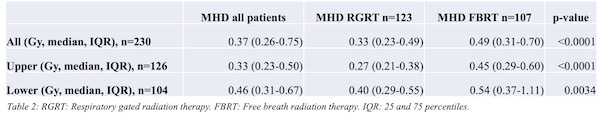
The median MHD for all left-sided PBI patients was 0.37 Gy, 0.33 Gy or upper located tumors and 0.46 Gy for lower located tumors. The median MHD for RGRT and FBRT was 0.27 Gy and 0.45 Gy respectively for upper located tumors and 0.40 Gy and 0.54 Gy for lower located tumors (Table 2).
In absolute numbers, the use of RGRT resulted in a reduction in median MHD of 0.16 Gy for all patients treated with left-sided PBI, 0.17 Gy for upper located tumors and 0.14 Gy for lower located tumors.
Of the evaluated 230 patients, 15 patients (6.5%), three RGRT and twelve FBRT, had a MHD >1.5 Gy. Of these 15 patients, eight had a tumor located in the upper part of the breast, 7 in the lower. Six patients (2.6%) had a MHD >2.5 Gy, two were treated with RGRT, four with FBRT.
Conclusion
For patients treated with left-sided PBI there is a significant reduction of MHD by using RGRT independent of tumor location. However, the absolute reduction in MHD is likely of no clinical relevance for the main part of the patients. Patients treated with FBRT were overrepresented in the group of patients with a MHD > 1.5 Gy. Thus, the gain of respiratory gating in PBI may still be clinically relevant in a few selected patients.