Salvage low-dose-rate brachytherapy for locally recurrent prostate cancer after radiotherapy
OC-0628
Abstract
Salvage low-dose-rate brachytherapy for locally recurrent prostate cancer after radiotherapy
Authors: Yannis Meraouna1, Pierre Blanchard2, Sandra Losa3, Alain Labib1, Samar Krhili1, Gilles Crehange1, Thierry Flam4, Jean-Marc Cosset5, Manon Kissel1
1Institut Curie, Radiotherapy, Paris, France; 2Gustave Roussy, Radiotherapy, Villejuif, France; 3Institut Curie, Physics, Paris, France; 4Clinique Saint Jean de Dieu, Urology, Paris, France; 5Centre Charlebourg - La Defense - Amethyst Radiothérapie, Radiotherapy, La Garenne-Colombes, France
Show Affiliations
Hide Affiliations
Purpose or Objective
The optimal management of locally recurrent prostate cancer after radiotherapy is still unclear but local salvage treatments are gaining interest. A retrospective, single-institution analysis of clinical outcomes and treatment-related toxicity in patients treated with salvage I-125 low-dose-rate (LDR) brachytherapy (BT) for locally-recurrent prostate cancer after radiotherapy was conducted in a Comprehensive Cancer Center.
Material and Methods
A total of 94 patients with an isolated local relapse of prostate cancer after radiotherapy who underwent salvage LDR-BT between 2006 and 2021 were included.
Results
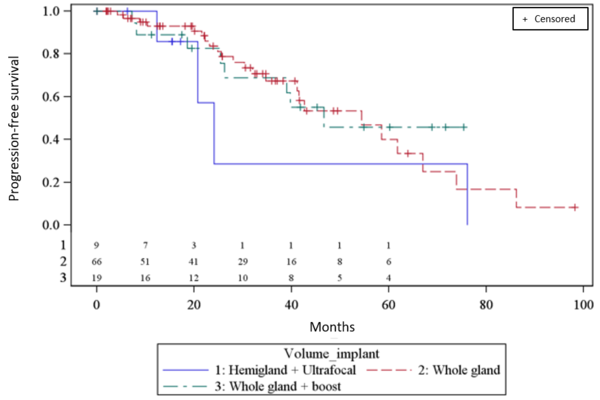
Median follow-up was 34 months. Initial radiotherapy was external beam radiotherapy in 73 patients (78%) with a median dose of 76 Gy [Q1-Q3: 74-76] and I-125 BT in 21 patients (22%) with a prescribed dose of 145 Gy. Median PSA at salvage brachytherapy was 3.75ng/mL [Q1-Q3: 2.4-5.9] with a median interval between first and salvage irradiation of 9.4 years [Q1-Q3: 6.7-11.7]. Histological proof of local relapse was available for all patients but one. Salvage LDR-BT was administered to either the whole gland (70%) with a dose prescription of 120 Gy for a large majority of the patients; the whole gland with a boost (20%) with a dose prescription of 90 Gy to the whole gland and 145 Gy to an MRI-based GTV; or a partial volume (hemigland or ultrafocal) (9%) with a dose prescription of 120 Gy (or 145 Gy for 1 patient only). It was associated with androgen deprivation therapy for 32% of the patients. Only 4% of the patients were castrate-resistant. Failure free survival (biological and clinical) was 82% and 66% at 2 and 3 years respectively in the whole population. The only factors associated with failure-free survival on multivariate analysis were hormonosensitivity at relapse and European Association of Urology (EAU) prognostic group. Late grade 3 urinary and rectal toxicities occurred in 12% and 1% of the patients respectively.
No significant difference in toxicity or efficacy was observed between the three implant volume groups.
Conclusion
The efficacy and toxicity results are consistent with available data and in particular with the LDR group of the MASTER meta-analysis published in 2020 (1). Salvage BT seems to be an effective and safe option for locally recurrent prostate cancer. A focal approach in this context could be interesting to reduce late severe toxicities, especially urinary, but data on large studies are lacking to establish its efficacy.
(1) Valle L.F., Lehrer E.J., Markovic D., et. al.: A systematic review and meta-analysis of local salvage therapies after radiotherapy for prostate cancer (MASTER). Eur. Urol. 2020; S0302283820308745Doi: