Dose and fractionation for palliative lung radiotherapy: 8 years of clinical practice
Charlotte Kristiansen,
Denmark
OC-0612
Abstract
Dose and fractionation for palliative lung radiotherapy: 8 years of clinical practice
Authors: Charlotte Kristiansen1, Thomas Leth Fink2,3, Torben Schjødt Hansen3, Mikkel Drøgemüller Lund3, Rune Slot Thing3
1Department of Oncology, Lillebaelt Hospital, Vejle, University Hospital of Southern Denmark, Vejle, Denmark; 2Institute for Regional Health Research, University of Southern Denmark, Vejle, Denmark; 3Department of Oncology, Lillebaelt Hospital, University Hospital of Southern Denmark, Vejle, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
In Denmark, about 50% of all new lung cancer patients are diagnosed with metastatic disease, and palliative radiotherapy (RT) is a very common treatment prescribed to this group of patients. Furthermore, palliative RT can be prescribed to patients with locally advanced lung cancer who are unfit for long course chemo-radiation. Palliative RT is therefore used both as first line treatment for some patients, and to relieve symptoms for other patients. Previous studies have shown that a substantial number of patients die before they achieve effect of palliative RT (i.e. 2 months), and for palliative RT, the optimal dose/fractionation schedule for lung cancer patients remains debated.
Material and Methods
We performed a retrospective analysis of our practice for palliative RT for lung cancer patients, delivered to the thoracic region only, from 2014 to 2021. Our RT department treats around 1800 RT courses per year, of which 100-150 are palliative treatments in the thorax. Looking only at patients with lung cancer as primary diagnosis, we counted the number of treatments prescribed per year per dose/fractionation (8Gy/1F, 20Gy/4F, 20Gy/5F, 30Gy/10F and 39Gy/13F).
The second part of the study focused on “long-term palliative RT”, i.e. 30Gy/10F and 39Gy/13F. A recent study from another center in Denmark showed no effect on overall survival when comparing 39Gy/13F to 30Gy/10F. As part of this study, we wanted to investigate if the same result emerged in our patient population. To ensure comparable patient characteristics, only patients with M0 disease where the entire tumor was irradiated were included in this part of the study.
Results
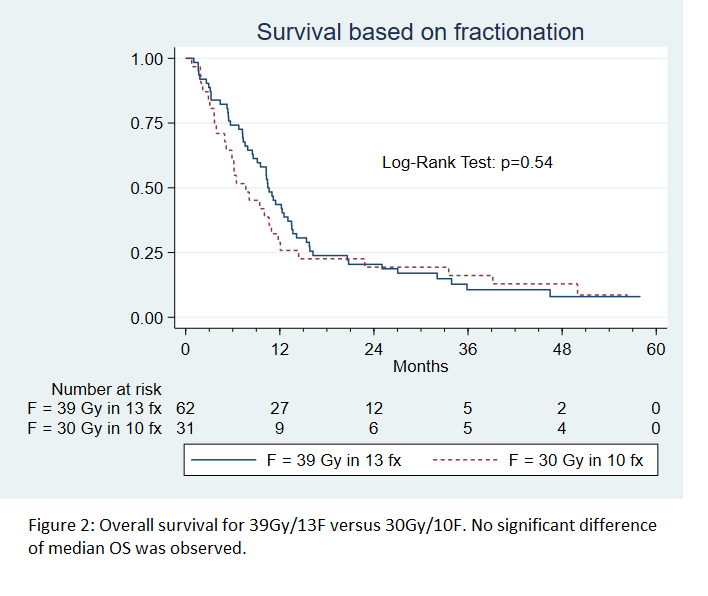
Figure 1 shows the distribution of palliative RT regimens prescribed per year in our department. For the last three years, fewer patients have been offered long-term palliative RT (10 or 13 fractions). Over the combined period, 62 patients were treated with 39Gy/13F, while 31 patients with similar characteristics were treated with 30Gy/10F. Figure 2 shows the survival curves for the two patient groups, with no difference observed in median overall survival (10.5 months and 7.7 months respectively, (p=0.5)). One patient died within the first 30 days, and 13% died within the first 90 days.

Conclusion
Practice has changed in our department over the last 8 years, with fewer patients being offered long-term palliative RT. With the realization, that 39Gy/13F offer no benefit in OS, this treatment regime is no longer offered at our institution. The change towards shorter RT courses is likely in part due to the COVID pandemic, which presented a demand for short course RT with few appointments for each patient. We do however believe that the increased use of short course RT based on improved patient selection, is to the benefit of elderly and frail patients, who will spend less time in the hospital and may suffer less toxicity compared to long course RT.