Evaluation of the dosimetric impact of PET-based adaptive radiotherapy in the PEARL Clinical Trial
Thomas Rackley,
United Kingdom
OC-0622
Abstract
Evaluation of the dosimetric impact of PET-based adaptive radiotherapy in the PEARL Clinical Trial
Authors: Mererid Evans1, Thomas Rackley2, Salvatore Berenato3, Owain Woodley3, Rebecca Windle3, Rhydian Maggs3, John Staffurth1, Sarah Hargreaves4, Phillip Wheeler3
1Cardiff University, Division of Cancer and Genetics, Cardiff, United Kingdom; 2Velindre University NHS Trust, Clinical Oncology, Cardiff, United Kingdom; 3Velindre University NHS Trust, Radiotherapy Physics, Cardiff, United Kingdom; 4Bristol Haematology and Oncology Centre, Clinical Oncology, Cardiff, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
PEARL is an ongoing, UK multi-centre clinical trial of adaptive, toxicity-sparing radiotherapy (RT) in patients with Stage I/II Human Papillomavirus (HPV)-positive oropharyngeal cancer. Patients receive a total dose of 66Gy in 33 fractions over 6 weeks, delivered in 2 phases using Volumetric Modulated Arc Therapy (VMAT). Adaptation is based on metabolic primary tumour response, visualised on a planning 18-FDG-PET CT scan carried out after 2 weeks chemoRT (10 fractions RT, 1 cycle Cisplatin). The adapted plan is implemented in Phase II, for the final 18 fractions of RT. This sub-study was conducted to evaluate the dosimetric impact of adaptation.
Material and Methods
For the first 10 recruited patients, automated planning was used to generate i) phase II PET-adapted RT plans as per the PEARL protocol and ii) standard, non-adapted plans for comparison. Both were planned to 38.7Gy in 18 fractions. Dosimetric comparison of Adapted vs Non-Adapted plans was performed for Swallowing Organs at Risk (SWOARS) and parotid glands; analysis was performed using Wilcoxon analysis. EdgeVCC, an automated planning system developed at Velindre Cancer Centre, Cardiff, was used to generate Adapted and Non-Adapted plans for each patient.
Results
Adapted, PET-based RT significantly reduced absorbed doses to the Superior and Middle Pharyngeal Constrictor Muscles (PCM_Superior, PCM_Middle) and Supraglottic Larynx (Larynx_SG), with no detriment to other OARs. Adaptation led to minor reductions in mean dose metrics to these organs overall (<1.2 Gy), but substantial reductions in higher Dose Volume Histogram (DVH) metrics (V30Gy, V35Gy, V38.7Gy), most notably V35Gy and V38.7Gy, with:
• V30Gy reduced by 4-7%
• V35Gy reduced by 11.8%, 11.1% and 12.1% for PCM_Superior, PCM_Middle and Larynx_SG respectively
• V38.7Gy reduced by 5.5%, 6.1% and 6.6% for PCM_Superior, PCM_Middle and Larynx_SG respectively
The impact of adaptation was patient dependent with respective ranges in the reduction of V35Gy of [1.3% to 28.2%], [-0.5% to 44.7%] and [0.0% to 51.6%] for PCM_Superior, PCM_Middle and Larynx_SG.
Table 1 compares OAR dose metrics for Adapted vs Non-Adapted treatment plans.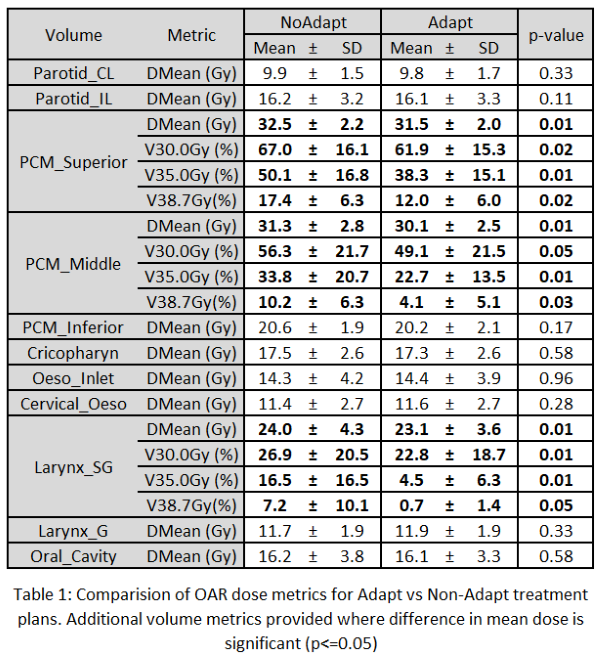
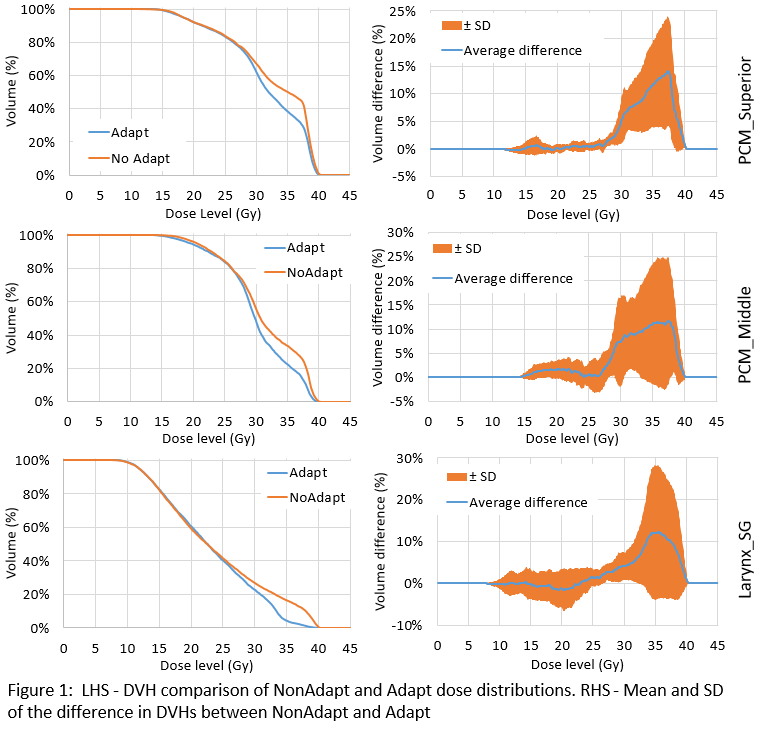
Figure 1 shows DVH comparison of Adapted vs Non-adapted dose distributions and the mean and Standard Deviation (SD) of the difference in DVHs.
Conclusion
PET-based adaptation, 2 weeks into a course of CRT, reduced doses to the SWOARS in close proximity to the oropharynx. Mean dose reduction to these organs was small, however substantial reductions were seen in high dose DVH metrics, approximating the range that is associated with development of long-term dysphagia. Ongoing recruitment and collection of late toxicity data in PEARL will determine the impact of these dosimetric advantages of adaptation on clinical outcomes, including late dysphagia.