Real-time clinical decision-making using motion including dose calculation
Edmund Goodwin,
United Kingdom
OC-0278
Abstract
Real-time clinical decision-making using motion including dose calculation
Authors: Edmund Goodwin1, Bjoern Eiben1, Emilia Persson1, Simeon Nill1, Uwe Oelfke1
1The Royal Marsden Hospital and the Institute of Cancer Research, The Joint Department of Physics, Sutton, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
We have developed a framework for calculating real-time motion-including dose for Unity MR-Linac patients (Elekta AB, Stockholm). Using this framework we aim to predict whether to intervene during treatment. Intervention may be as simple as pausing delivery to wait for anatomy to revert to a baseline state, or may be complex, such as initiating online replanning. We investigate whether dose data provides a better basis for a prediction model than the motion data alone.
Material and Methods
18 prostate cancer patients (36.25Gy/5#) treated using 9 field IMRT on an MR-Linac were selected. The 3D centroid shift of the CTV was extracted from cine images taken during treatment using an optical flow algorithm. Motion-including and zero-motion real time dose reconstruction were performed as in [1]. After each beam, DVHs for clinical structures were calculated.
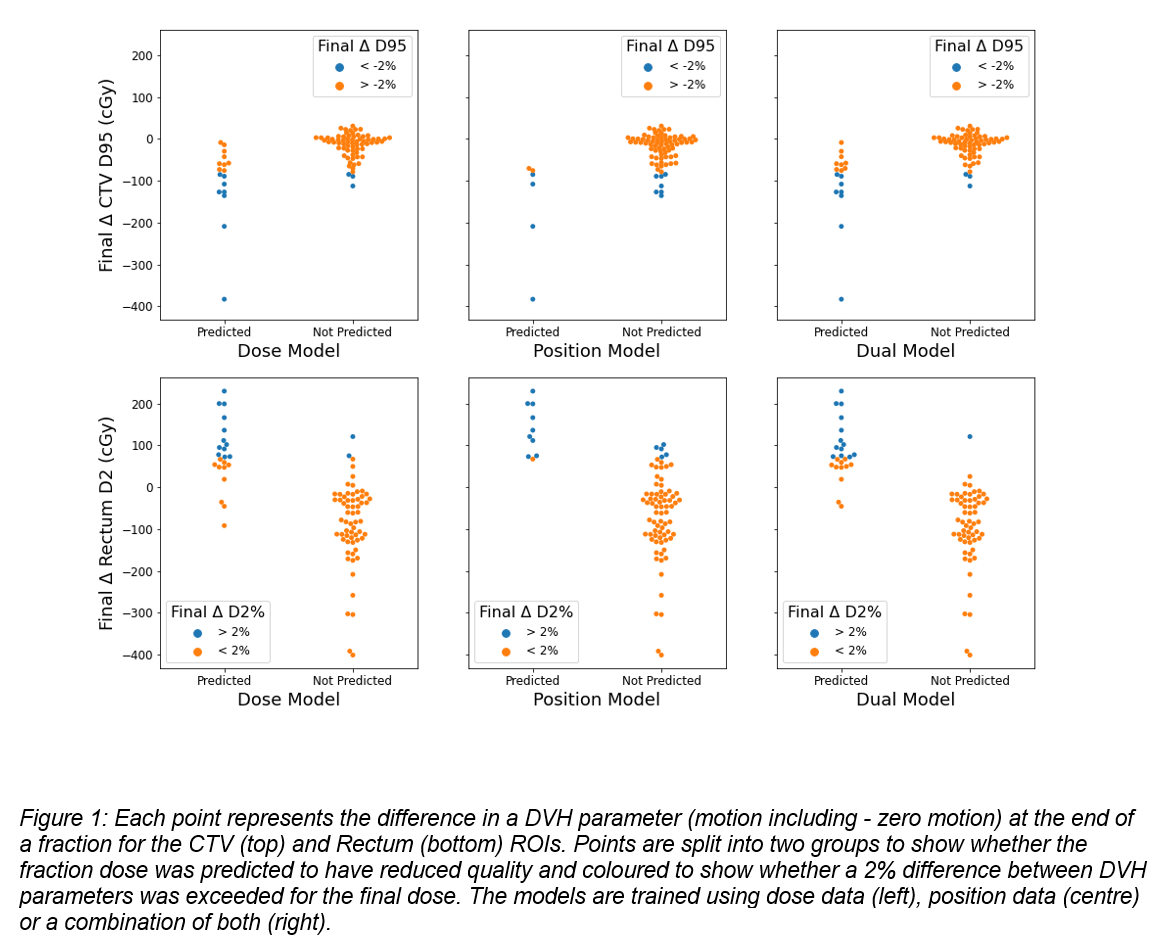
The CTV coverage and the near-maximum dose to the rectum were selected to determine dose delivery quality. Reduced quality was defined if the motion-including CTV D95% was more than 2% lower, or the rectum D2% more than 2% higher the zero-motion parameter at the end of treatment.
A model was made for each DVH parameter (DVHp). The models used 8 separate logistic regressions (LR) scored at the end of delivery of each of the first 8 beams to predict reduced quality. Three approaches to training the models were used: a dose model, using the DVHp for the current and all previous beams, a position model, using the average CTV position during delivery of each beam up to the current, and a dual model, where both dose and position data were used.
The models were trained using a leave-one-out method on a per patient basis. If any of the LR predicted reduced quality with a probability >0.75, the overall result for that fraction was scored as reduced quality, and later beams were not assessed.
Results
For the dose, position, and dual models respectively the CTV D95 prediction sensitivities were 0.47, 0.67 and 0. 47, the specificities were 0.96, 0.91 and 0.96. The Rectum D2% prediction sensitivities were 0.55, 0.90 and 0.54 and specificities were 0.97, 0.93 and 0.98. Our goal was the detection of fractions with reduced quality, so specificity was the priority.
The three models predicted cases of reduced plan quality, though accurately predicting fractions where the 2% threshold in DVHp was exceeded was difficult (see fig. 1), likely due to the large amount of variability in patient motion.
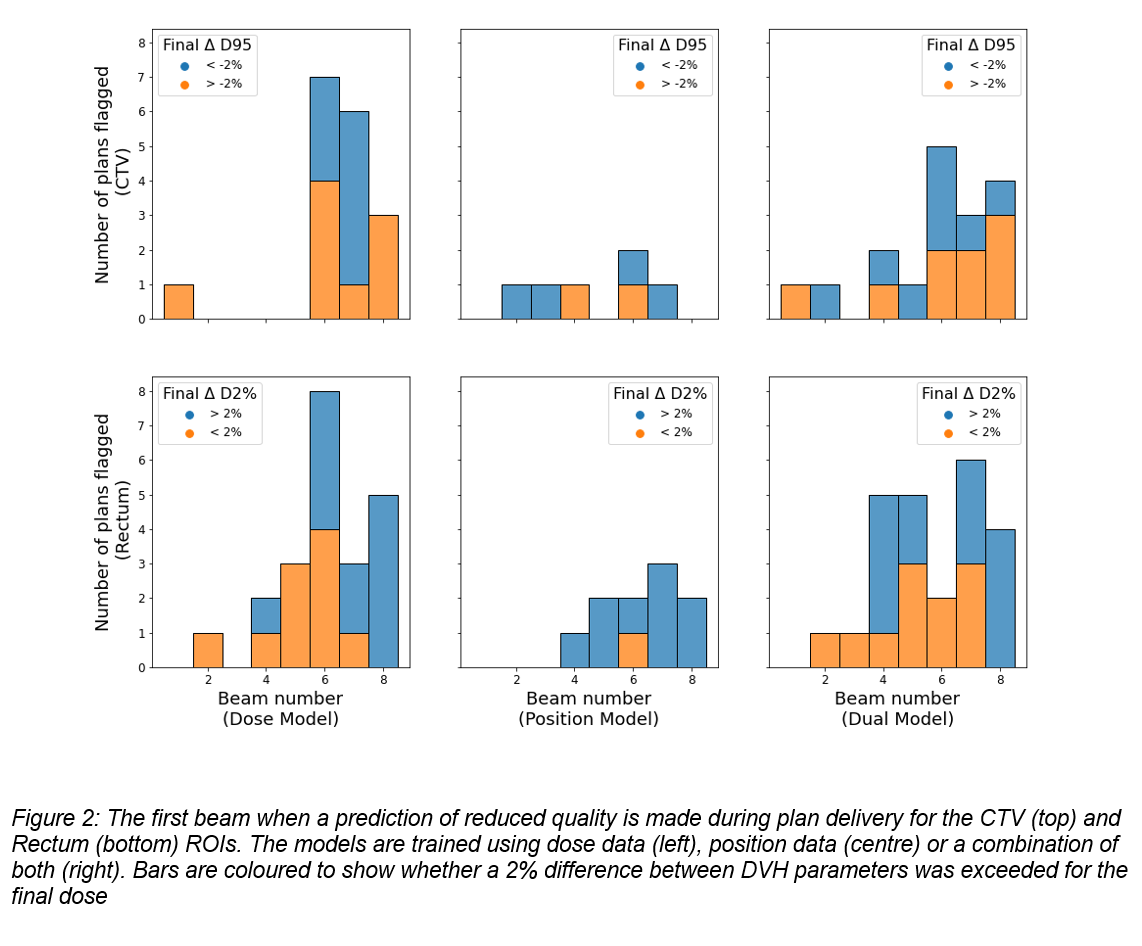
The dual model could predict reduced quality fractions earlier during treatment than the others (see fig. 2). This is desirable as it gives more scope for correction.
Conclusion
All models can detect which fractions are likely to have reduced quality due to motion-induced changes in dose. The dose model is preferable to the position model as it is more specific. The model utilising both dose and position data is best as it is most specific and it makes predictions earlier.
1) Goodwin, E., Real time motion-including dose reconstruction on the MR-Linac. ESTRO 2021