Relationships between microbiome and response to neoadjuvant chemoradiotherapy in rectal cancer
Hye In Lee,
Korea Republic of
OC-0276
Abstract
Relationships between microbiome and response to neoadjuvant chemoradiotherapy in rectal cancer
Authors: Hye In Lee1, Bum-Sup Jang1, Ji Hyun Chang1, Tae Hoon Lee1, Jeong Hwan Park1, Eui Kyu Chie1
1Seoul National University Hospital, Department of Radiation Oncology, Seoul, Korea Republic of
Show Affiliations
Hide Affiliations
Purpose or Objective
Gut microbiome is known to be involved in antitumor immunotherapy and chemotherapy responses; however, few research has focused on the role of gut microbiome in the setting of concurrent chemoradiotherapy (CCRT). In this study, we investigated the tumor microbiome dynamics in patients undergoing neoadjuvant CCRT for locally advanced rectal cancer and sought to determine whether the diversity and composition of microbiome affect treatment response.
Material and Methods
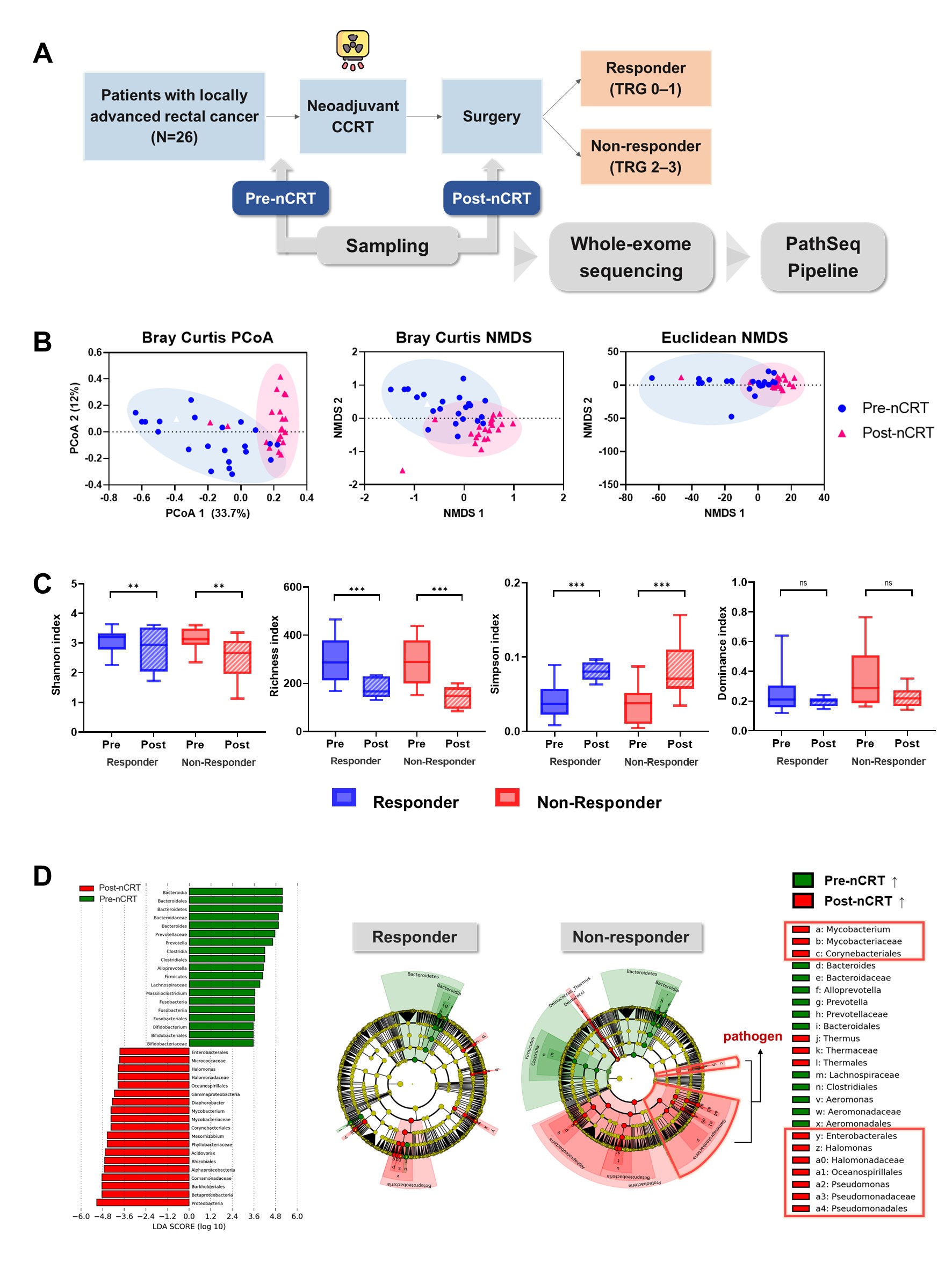
A total of 103 samples from 26 patients with locally advanced rectal cancer were collected and 16S ribosomal RNA amplicon sequencing was performed. All patients underwent neoadjuvant CCRT followed by surgical resection between 2008 and 2016. Samples were obtained from both tumor and normal rectal tissue at pre- and post-CCRT. According to the American Joint Committee on Cancer tumor regression grading (TRG) system, patients were divided into responders (TRG 0, 1) and non-responders (TRG 2, 3). We performed diversity, taxonomy, and network analyses to compare responders and non-responders. Then, we established the Bayesian network model to predict treatment response in patients with rectal cancer.
Results
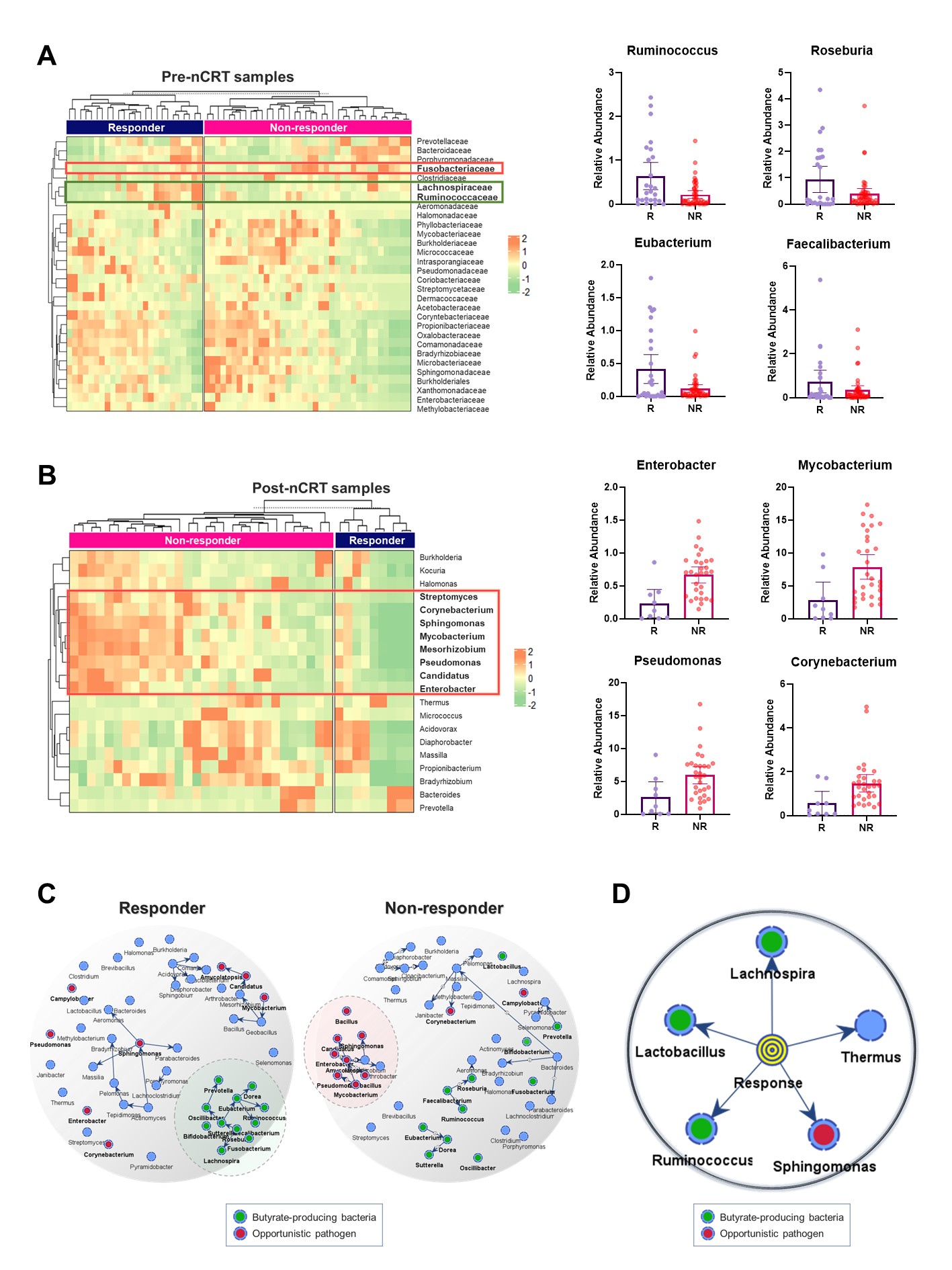
Overall, we detected 1260 microbial genera from 287 families, 132 orders, 56 classes, and 32 phyla in the bacteria kingdom. Between tumor and normal rectal tissues, there was no difference in microbial diversity and composition. On the other hand, there was a significant decrease in diversity and compositional alterations when comparing pre- and post-CCRT samples (all p<0.001). Ten patients (38.5%) were classified as responders and 16 patients (61.5%) were classified as non-responders. In both groups, CCRT significantly reduced microbial diversity and altered their composition, but it was more pronounced in non-responders. In taxonomic analysis of pre-CCRT samples, butyrate-producing bacteria were differentially enriched in responders. Meanwhile, in post-CCRT samples, opportunistic pathogen were overrepresented in non-responders. The network analysis revealed that butyrate-producing bacteria had strong interactions in responders, whereas opportunistic pathogen demonstrated strong interactions in non-responders (Pearson’s coefficient>0.5). Finally, five microbes were selected as the optimal set for the response prediction model, which yielded an area under the curve value of 82.33%.
Conclusion
CCRT significantly changed the diversity and composition of microbiome, especially in non-responders. Several microbes might be related with treatment response. These findings highlight the potential of microbiome to play an important role as a biomarker in patients with rectal cancer.
[Figure 1]
[Figure 2]