Development of a comprehensive 4DCT QA program: Implementation and validation
Jinane Bakkali Tahiri,
Belgium
PD-0581
Abstract
Development of a comprehensive 4DCT QA program: Implementation and validation
Authors: Jinane Bakkali Tahiri1,2, Manuela Burghelea1, Martin Kyndt3, Akos Gulyban1, Jennifer Dhont4, Sziktsak Juliane5, Evelien Bogaert6, Dirk Van Gestel7, Nick Reynaert7
1Jules Bordet Institute, Medical Physics, Radiotherapy, Brussels, Belgium; 2GasthuisZusters Antwerpen Ziekenhuizen, Medical Physics, Radiotherapy, Antwerp, Belgium; 3MIM Software, Workflow, Genk, Belgium; 4Jules Bordet Institute, Data science, Brussels, Belgium; 5Universitätsklinikum Erlangen, Department of Radiation Oncology, Erlangen, Germany; 6Ghent University Hospital, Department of Radiotherapy-Oncology, Ghent, Belgium; 7Jules Bordet Institute, Radiation Oncology Department, Brussels, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
As artifacts in 4DCT were shown to negatively influence clinical outcome after SBRT, this study aimed to develop and validate a comprehensive but easily executable automatic 4DCT QA program that evaluates image accuracy and consistency across different breathing patterns.
Material and Methods
The Thorax dynamic phantom (CIRS, Norfolk, USA) with imaging insert (2cm diameter “tumor” sphere) was selected for all tests. Five regular and three irregular breathing patterns (double amplitude (DA), irregular frequency (IF) and irregular breathing (IB)) were created combining various amplitudes (2.5-25mm) and periods (2.8-7s). 4DCT scans were acquired using the i4DCT algorithm clinically implemented on our SOMATOM go.Open Pro scanner (Siemens Healthcare, Germany), used in conjunction with the RGSC monitoring system. For each test, a 3DCT, 10-phase 4DCT, maximum - (MaxIP) and average intensity projection (AvgIP) were reconstructed.
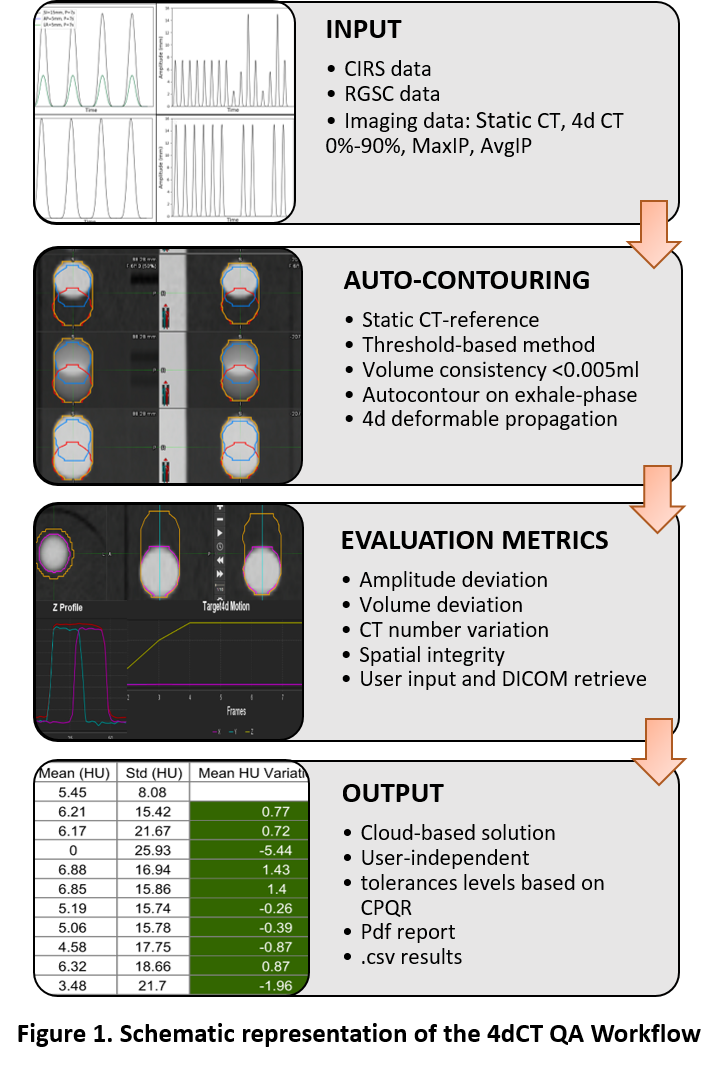
Based on the Canadian Partnership for Quality Radiotherapy (CPQR) recommendations, an automatic 4DCT evaluation workflow was developed in MIM Maestro (MIM Software, CLE, USA) focusing on volume and amplitude deviation, CT HU number accuracy, and spatial integrity (Figure 1). The corresponding tolerances were pre-configured for each parameter (<5%, <2mm and <10HU, respectively) and the 3DCT acquired without phantom motion served as ground truth.
To evaluate the repeatability of the workflow, each measurement was repeated three times.
Results
The monitoring system correctly detected the motion with an accuracy better than 1mm.
High consistency was observed for HU deviation and volume deviation across repetitions, where the tolerances were respected in all tests (mean <10HU and <5%, respectively).
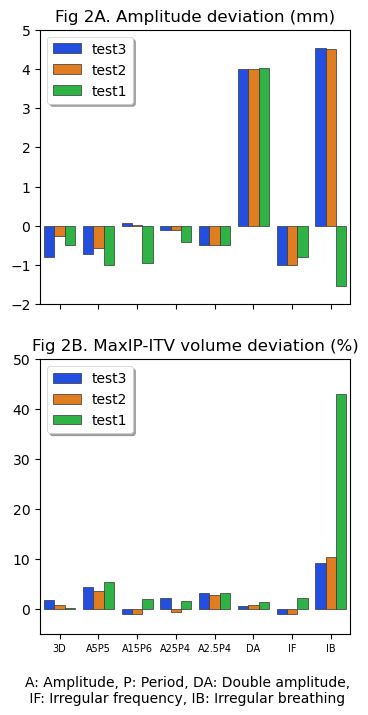
For all breathing patterns, the correct motion amplitude was captured by the 4DCT, with deviations from the ground truth smaller than 0.5mm in all three directions, except for DA and IB curves (Figure 2A) that simulate extreme cases. These curves' reconstructed amplitude was dependent on when the acquisition was started (at the high or low amplitude peak).
MaxIP scans (reconstructed in Siemens software) showed the expected volume in SI direction with a MaxIP-ITV volume deviation below 5% for all tests except for the IB where MaxIP was overestimating the movement by 40% (Figure 2B). MaxIP did not overestimate the ITV when it was reconstructed in MIM. This could be explained by the fact that Siemens uses raw data and MIM uses imaging data for the reconstruction.
Conclusion
Our protocol (using regular and irregular breathing motion patterns) allows us to perform a comprehensive QA workflow of 4DCT imaging and is capable of detecting and quantifying image quality degradation following the CPQR recommendations. The automated workflow allows easy and standardized reporting. Additionally, the repeatability test confirms the robustness of the QA procedure, which initiated an ongoing multi-centric QA audit.