Radiation-induced lymphopenia risk model predicts durvalumab benefit in non-small cell lung cancer.
PD-0152
Abstract
Radiation-induced lymphopenia risk model predicts durvalumab benefit in non-small cell lung cancer.
Authors: Peter van Rossum1, Pim Damen2,1, Ting Xu1, Brian Hobbs3, Radhe Mohan4, Zhongxing Liao1, Steven Lin1
1The University of Texas MD Anderson Cancer Center, Radiation Oncology, Houston (TX), USA; 2UMC Utrecht, Radiation Oncology, Utrecht, The Netherlands; 3The University of Texas at Austin, Population Health, Dell Medical School, Austin (TX), USA; 4The University of Texas MD Anderson Cancer Center, Radiation Physics, Houston (TX), USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Severe radiation-induced lymphopenia (RIL) in patients undergoing concurrent chemoradiotherapy (CRT) for non-small cell lung cancer (NSCLC) is associated with decreased immunotherapy efficacy and survival. Severe RIL mostly occurs in the final weeks of CRT, when it is too late for meaningful modification of RT plans or techniques for lymphocyte-sparing. Therefore, a prediction model that identifies patients at high risk of severe RIL before treatment (i.e. a-priori) is warranted. The primary aim of this study was to develop and validate a nomogram based on pretreatment predictors for severe RIL. A secondary aim was to assess the survival impact of adjuvant durvalumab for different RIL risk groups.
Material and Methods
Patients who underwent concurrent CRT for NSCLC between 2010 and 2019 were identified. Absolute lymphocyte counts (ALCs) were obtained prior to, and weekly during CRT. Severe RIL was defined as a lowest ALC during CRT (ALCnadir) of <0.24 K/µL. Multivariable logistic regression analysis was used to build a prediction model for severe RIL and internal validation was performed using bootstrapping. The model was evaluated in terms of discrimination and calibration, and presented as nomogram. For 2 nomogram risk groups, progression-free survival (PFS) and overall survival (OS) after durvalumab vs. no durvalumab were evaluated.
Results
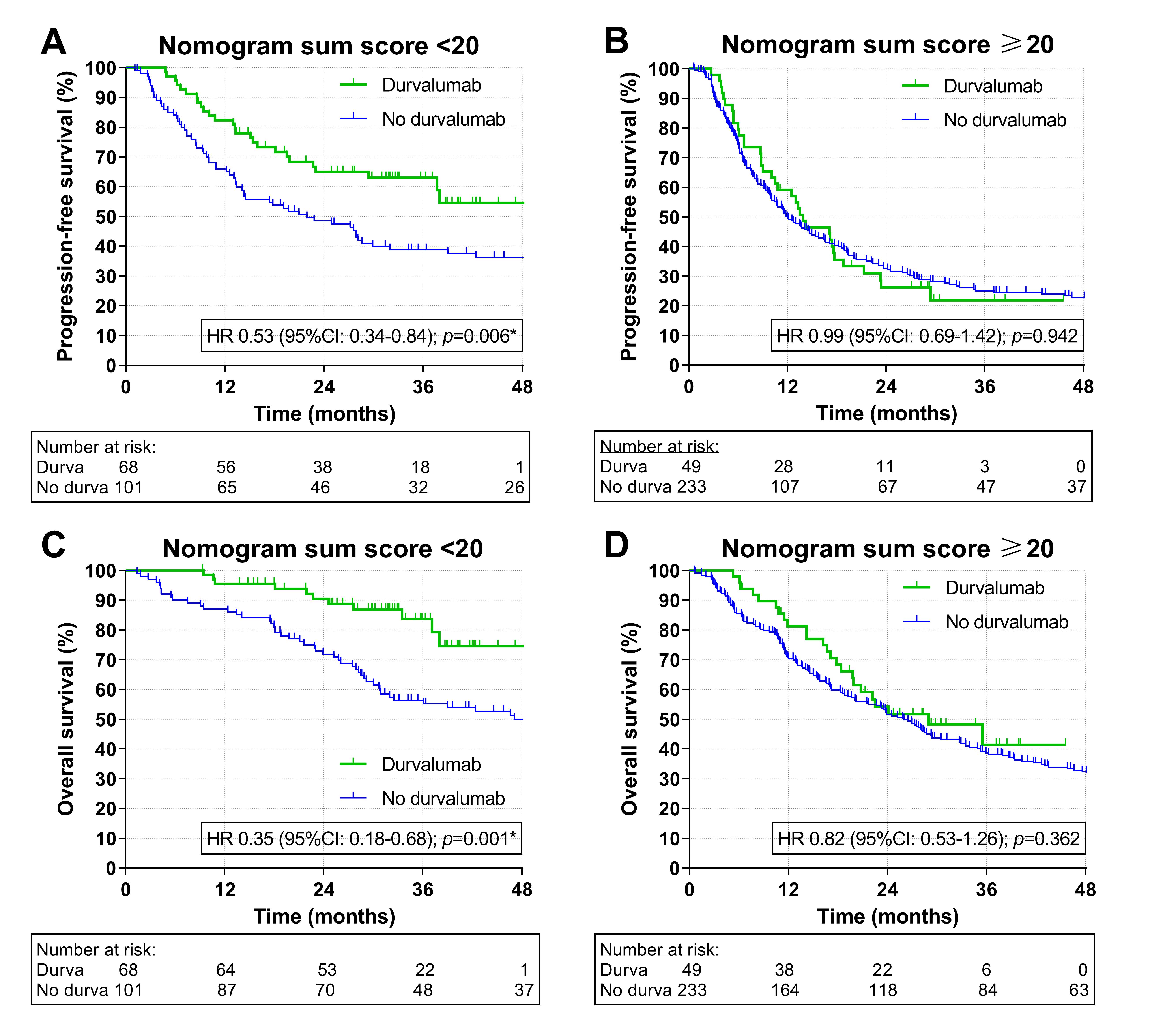
Among 451 included patients, 164 (36%) experienced severe RIL. Higher age, cN3-stage (vs. cN0-2 stage), larger planning target volume (PTV), >30 (vs. ≤30) RT fractions, higher mean lung dose (MLD), and lower baseline ALC were independently predictive for severe RIL in the final model. The discriminatory model performance was fair with a corrected c-statistic (after internal validation) of 0.70 (95%CI: 0.65-0.75). Model calibration among risk quintiles was excellent with mean predicted risks of severe RIL of 15%, 26%, 35%, 45%, and 62%, corresponding to observed risks of 13%, 26%, 37%, 43%, and 63%, respectively. A nomogram was created with a sum score ranging from 0 to 40 (Fig. 1). Among 169 patients with a nomogram sum score <20, adjuvant durvalumab was administered in 68 (40%). In these patients with a low predicted risk of severe RIL, durvalumab (vs. no durvalumab) yielded a significantly improved PFS (Fig. 2A; p=0.006) and OS (Fig. 2C; p=0.001). In contrast, among the 282 patients with a high predicted risk of severe RIL (nomogram sum score ≥20), adjuvant durvalumab in 49 patients (17%) demonstrated no superiority in terms of PFS (Fig. 2B; p=0.942) or OS (Fig. 2D; p=0.362).
Fig. 1
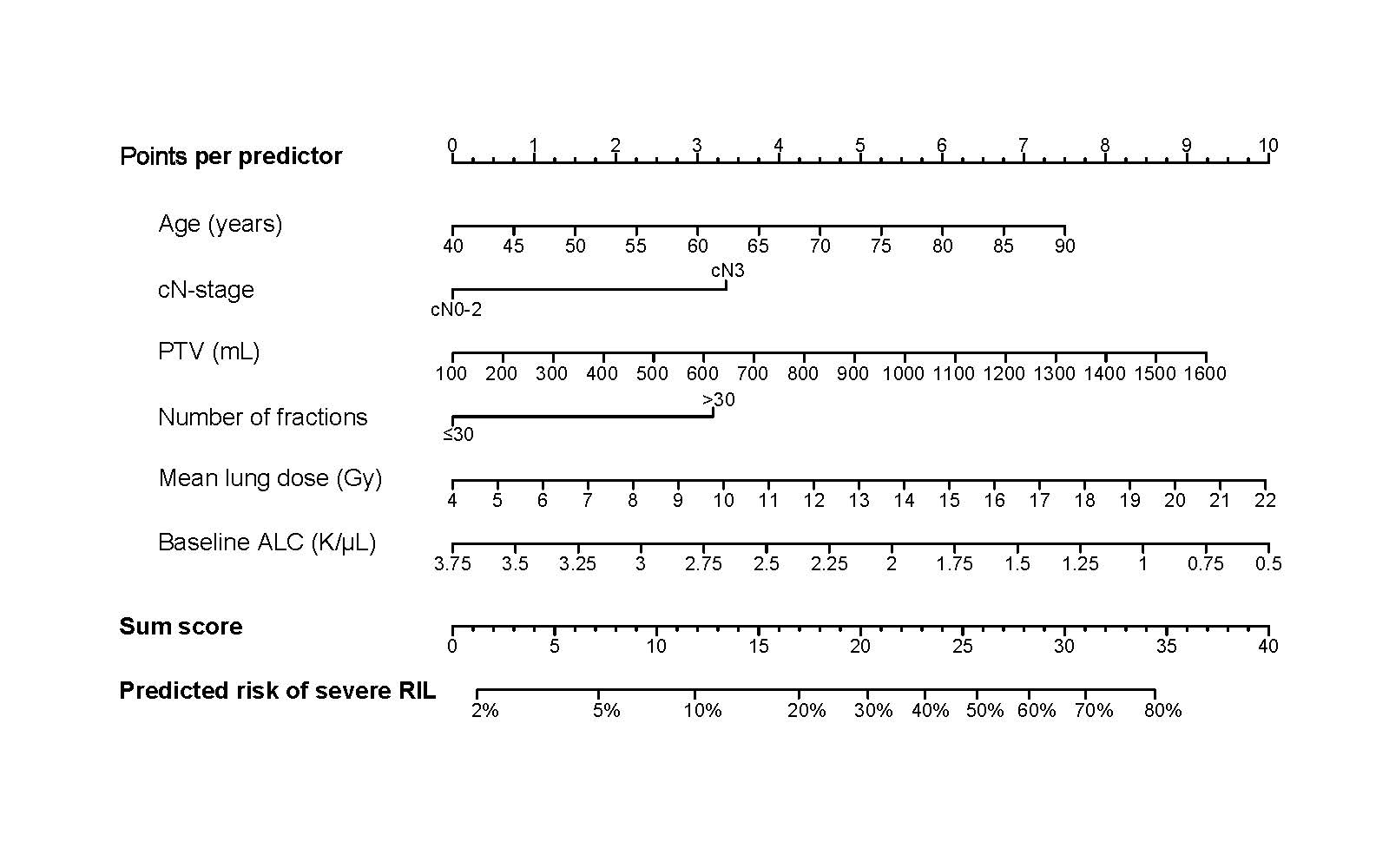
Fig. 2
Conclusion
A pretreatment model to predict severe RIL during CRT for NSCLC was developed and validated internally. Adjuvant durvalumab benefit was observed in patients with a low predicted risk of severe RIL, but not in patients with a high predicted risk. Therefore, this prediction model has the potential to enable accurate selection of high-risk patients who may benefit from lymphopenia-mitigating strategies to improve immunotherapy efficacy and survival.