Multisector dosimetric analysis to determine in-vivo dosimeter positions in prostate brachytherapy.
Orla Houlihan,
United Kingdom
PD-0417
Abstract
Multisector dosimetric analysis to determine in-vivo dosimeter positions in prostate brachytherapy.
Authors: Orla Houlihan1,2, Sergio Esteve3, Owen McLaughlin2,3, Geraldine Workman3, Monica Byrne3, Kevin Prise2, Alan Hounsell3, Darren Mitchell1, Suneil Jain1,2
1Northern Ireland Cancer Centre, Belfast Health and Social Care Trust, Clinical Oncology, Belfast, United Kingdom; 2Queen’s University Belfast, Patrick G. Johnston Centre for Cancer Research, Belfast, United Kingdom; 3Northern Ireland Cancer Centre, Belfast Health and Social Care Trust, Radiotherapy Medical Physics, Belfast, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
To determine the optimal positions within the prostate for in vivo dosimeters, developed as part of the EU H2020 Origin project, using multisector dosimetric analysis to optimise brachytherapy delivery.
Material and Methods
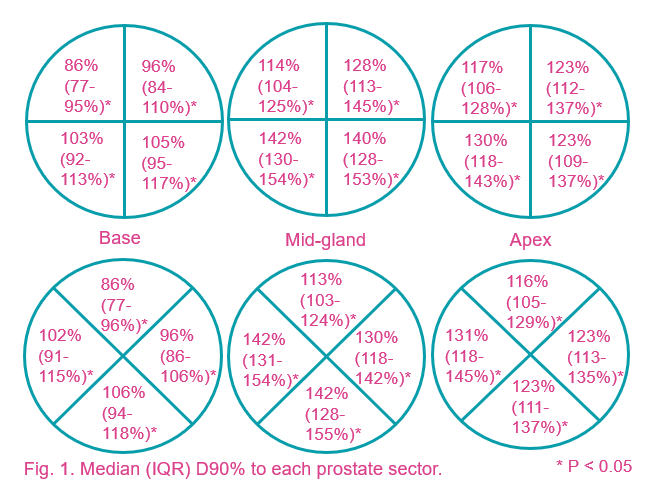
Dosimetric data from post-implant CTs were obtained for 611 men treated with LDR prostate brachytherapy 2009-2020. Sectors were created by dividing the prostate into three equal thirds (base/midgland/apex), then each third into four axial sectors. Axial division was performed by two separate methods; plus-shape (“+”) and cross-shape (“x”). Dose to 90% of each sector (D90%) was compared to D90% of the global prostate gland for each method.
Results
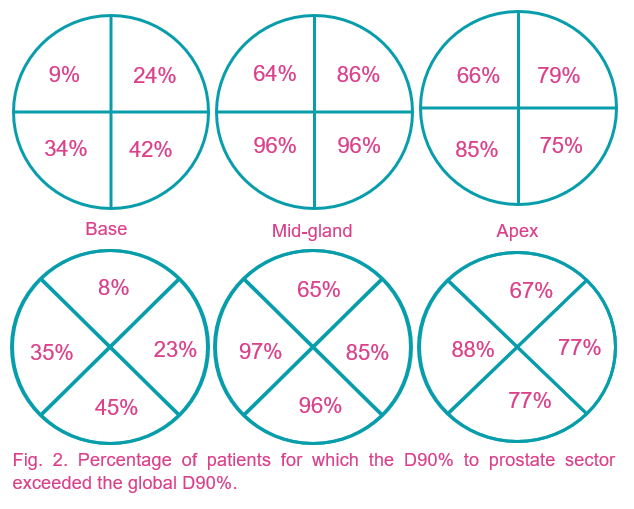
Compared to the median global D90% of 108% (interquartile range (IQR) 102-114%), median D90% of the anterior right base was lowest (86%, IQR 77-95%) and the anterior left base was second lowest (96%, IQR 84-110%) using the plus-shaped sector division (Fig. 1), with the D90% < global D90% in 91% and 76% of cases respectively (Fig. 2). Using the cross-shaped sector division, median D90% of the anterior and left base were lowest at 86% (IQR 77-96%) and 96% (IQR 86-106%) respectively (Fig. 1) with D90% < global D90% in 92% and 77% of cases respectively (Fig. 2).
The posterior right and left mid-gland sectors had the highest median D90% at 142% and 140% (IQR 130-154% and 128-153% respectively) using the plus-shaped sector division (Fig. 1), with the D90% > the global D90% in 96% of cases for both sectors (Fig. 2). Using the cross-shaped sector division, the right and posterior mid-gland sectors received the highest median dose at 142% (IQR 131-154% and 128-155% respectively) (Fig. 1), with D90% > global D90% in 97% and 96% of cases respectively (Fig. 2).
Conclusion
The median D90% was lowest for the anterior base sectors and highest for the posterior mid-gland sectors with a significant percentage of the D90% of these sectors < or > global D90% respectively. Overlapping sectors with the highest differences of D90% from global D90% are appropriate locations for in-vivo dosimeters to monitor radiation dose.