In silico trial of CBCT-stereotactic adaptive radiation for the ultra-central thorax (NCT04008537)
PD-0749
Abstract
In silico trial of CBCT-stereotactic adaptive radiation for the ultra-central thorax (NCT04008537)
Authors: Joshua Schiff1, Eric Laugeman1, Hayley Stowe1, Xiaodong Zhao1, Jessica Hilliard1, Ellie Hawk1, Jesiah Watkins1, Casey Hatscher1, Shahed Badiyan1, Pamela Samson1, Geoffrey Hugo1, Alex Price1, Lauren Henke1
1Washington University School of Medicine in St. Louis, Department of Radiation Oncology, St. Louis, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
We conducted a prospective in silico study to evaluate the feasibility of CBCT-guided stereotactic adaptive radiotherapy (CT-STAR) for the treatment of ultra-central (UC) thoracic cancers. We hypothesized that CT-STAR would widen the dosimetric therapeutic index compared to non-adapted SBRT through improved organ-at-risk (OAR) sparing and maintained tumor coverage.
Material and Methods
Separate from their standard-of-care treatment on other clinical machines, patients receiving radiation for UC malignancies underwent 5 kV CBCTs on the ETHOS system as part of a prospective in silico imaging clinical trial. These images, collected on consecutive treatment fractions (fx) to best represent inter-fx anatomic changes, were then used to simulate daily adaptation using an emulator system. Initial plans (PI) were created based on simulation images and daily adaptive plans (PA) were based on the anatomy-of-the-day. The prescription dose was 55Gy/5fx. OAR constraints were prioritized over planning target volume (PTV) coverage using a strict isotoxicity approach. PI were applied to the patients’ daily imaging and compared to the re-optimized PA using DVH metrics. Feasibility was defined as completion of the adaptive workflow and compliance with strict OAR constraints in ≥ 80% of fx. Simulated fx were performed under time pressures.
Results
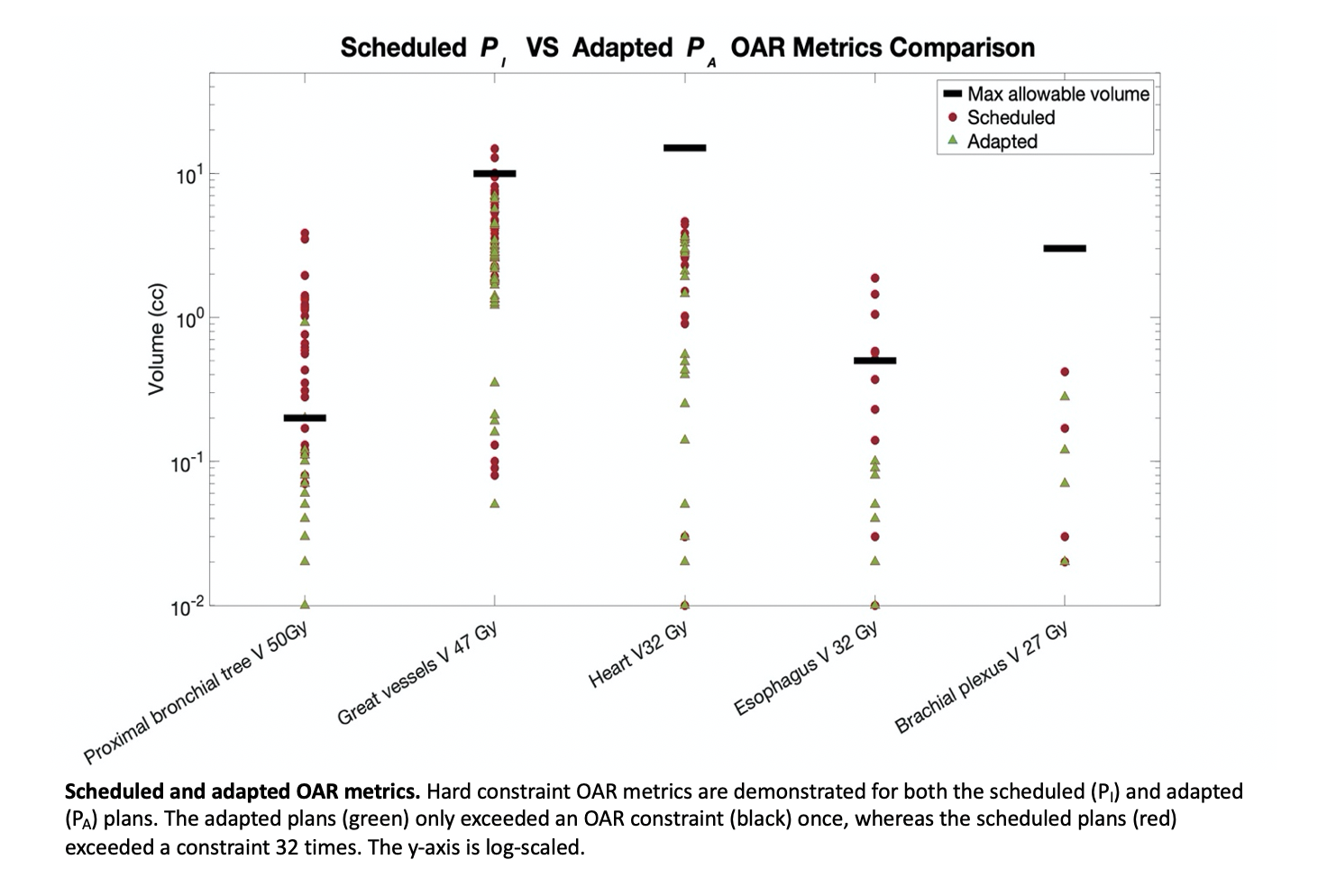
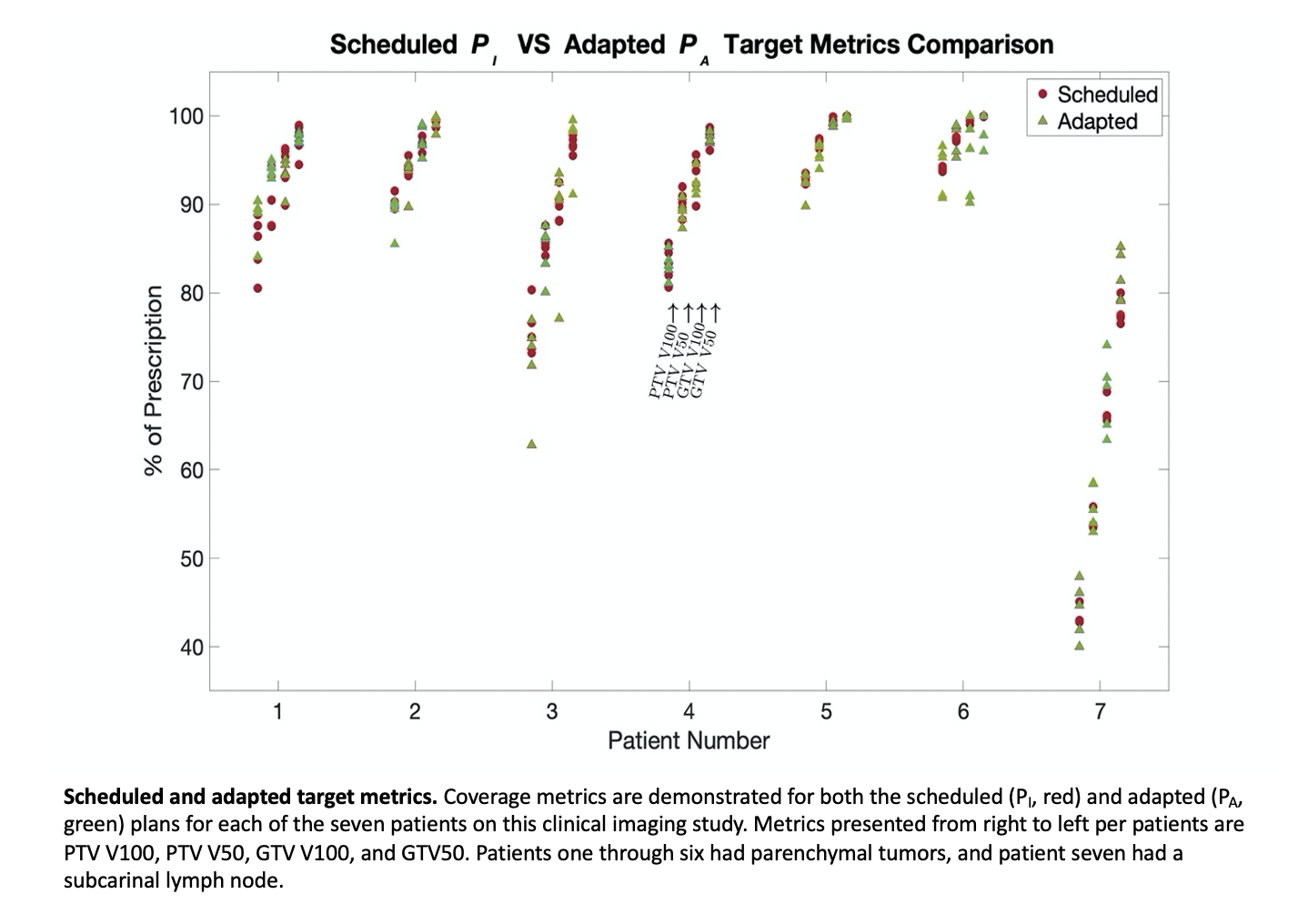
7 patients with UC lung tumors were accrued. CT-STAR was feasible in 34/35 simulated fx. 32 constraint violations occurred in the PI across 22/35 fx. These violations were resolved in the PA in all but 1 fx, in which the proximal bronchial tree constraint was still numerically improved from the PI to the PA. The mean difference between the PTV and GTV V100% in the PI and the PA was -0.24% (-10.40–9.90) and -0.62% (-11.00–8.00), demonstrating no significant decrease in target coverage. Mean total adaptive time was 28 minutes (18–51).
OAR
| Constraint
| # of PI constraint violations
| PI mean (range)
| PA mean (range)
|
Proximal Bronchial Tree
| V50Gy<0.20cc
| 22
| 0.74 (0.00–3.85)
| 0.08 (0.00-0.92)
|
Great Vessels
| V47Gy<10.00cc
| 3
| 4.65 (0.00–14.79)
| 2.43 (0.05–6.98)
|
Heart
| V32Gy<15.00cc
| 0
| 1.31 (0.00–4.63)
| 0.86 (0.00–3.61)
|
Esophagus
| V32Gy<0.50cc
| 6
| 0.19 (0.00–1.88)
| 0.01 (0.00–0.10)
|
Brachial Plexus
| V27Gy<3.00cc
| 0
| 0.02 (0.00–0.42)
| 0.01 (0.00–0.28)
|
Spinal Cord
| V25Gy<1.00cc
| 0
| 0.02 (0.00–0.35)
| 0.00 (0.00–0.01)
|
| Target Volume Metric | Goal | N/A
| PI mean (range)
| PA mean (range)
|
PTV V100%
| N/A
| N/A
| 80.67 (42.80–94.30)
| 80.43 (40.00–96.60)
|
PTV V50Gy
| N/A
| N/A
| 86.96 (53.50–97.60)
| 87.16 (53.00–98.90)
|
PTVopt D95%
| > 95%Rx
| N/A
| 54.30 (41.00–58.05)
| 57.15 (53.85–59.25)
|
GTV V100%
| N/A
| N/A
| 91.29 (65.60–99.90)
| 90.67 (63.40–100.00)
|
GTV V50Gy
| N/A
| N/A
| 95.54 (76.50–100.00)
| 95.98 (79.10–100.00)
|
*Data for non-critical OARs (uninvolved lung, chest wall) not shown.
Conclusion
CT-STAR resolved strict OAR constraints while maintaining adequate tumor coverage when compared to non-adapted SBRT plans for patients with UC thoracic tumors. A phase I prospective protocol is currently under development to evaluate the safety of this treatment planning paradigm for patients with UC early-stage NSCLC.