Anatomic pattern of recurrence after single or multifraction SBRT for lymph nodal lesions.
PD-0069
Abstract
Anatomic pattern of recurrence after single or multifraction SBRT for lymph nodal lesions.
Authors: Milena Ferro1, Gabriella Macchia1, Donato Pezzulla1, Savino Cilla2, Carmela Romano2, Marica Ferro1, Mariangela Boccardi1, Paolo Bonome1, Vincenzo Picardi1, Silvia Cammelli3,4, Milly Buwenge3, Alessio Giuseppe Morganti3,4, Francesco Deodato1,5
1Gemelli Molise Hospital – Università Cattolica del Sacro Cuore, Radiation Oncology Unit, Campobasso, Italy; 2Gemelli Molise Hospital – Università Cattolica del Sacro Cuore, Medical Physics Unit, Campobasso, Italy; 3IRCCS Azienda Ospedaliero-Universitaria di Bologna, Radiation Oncology, Bologna, Italy; 4Alma Mater Studiorum Bologna University, Department of Experimental, Diagnostic, and Specialty Medicine - DIMES, Bologna, Italy; 5Università Cattolica del Sacro Cuore, Istituto di Radiologia, Roma, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Single (SRS) or multi-fraction Stereotactic Body RadioTherapy (SBRT) are effective treatment options for the treatment of oligometastatic disease of lymph nodes. Despite the encouraging local control rate, progression-free survival remains unfair due to relapses that might occur in the same district or at other sites. The recurrence pattern analysis after nodal SRS/SBRT in oligometastatic patients could pave the way for different strategies of therapeutic intensification.
Material and Methods
This retrospective trial looks into the patterns of failure in patients with nodal metastases who were enrolled and treated with SBRT (DESTROY-1) or SRS (DESTROY-2) in 2 prospective trials at our Institution. We documented the various relapse locations of the involved lymph nodes that had been irradiated with a previous RT dose of 20 to 50 Gy in five daily fractions or 12 to 24 Gy single fraction treatment.
Results
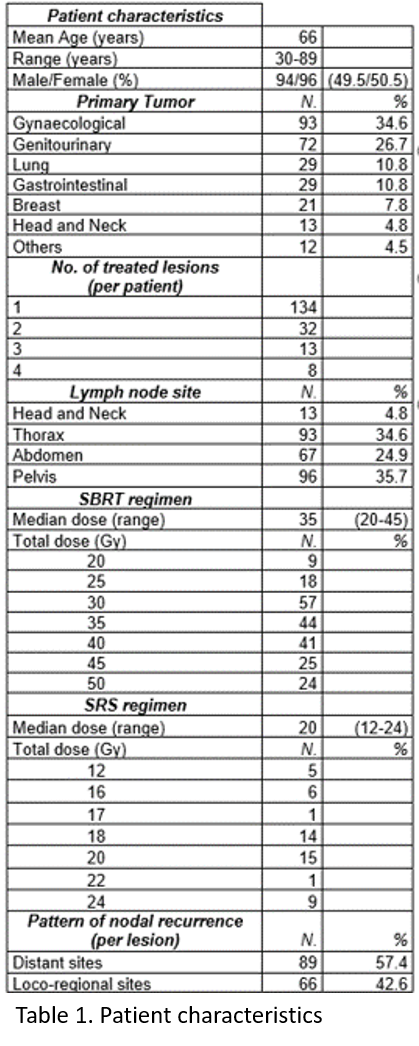
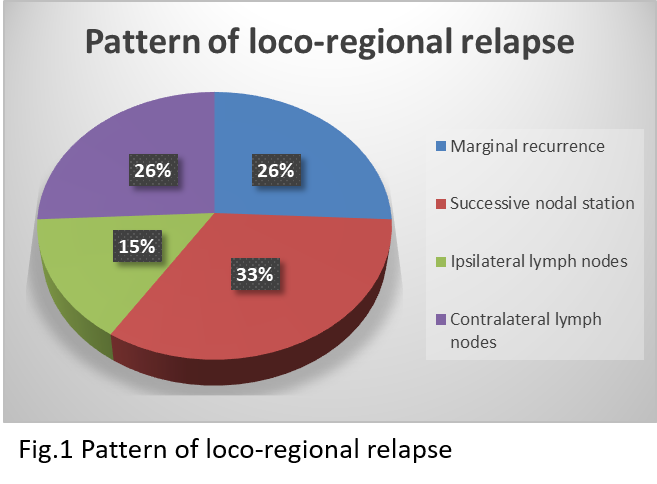
Data on 190 patients who received SBRT or SRS on 269 nodal lesions were reviewed. The male/female ratio was 94/96 and the median age was 66 years (range: 30-89). The most represented primary cancer was the gynaecological one (34.6%), followed by genitourinary cancer (26.7%). Pathologic lymph nodes were most frequently located in the pelvis (35.7%), followed by the thorax (34.6%) and the abdomen (24.9%) (Table 1). After SBRT/SRS the recurrences were diagnosed at imaging with a median distant metastasis-free survival (DMFS) time of 17 months (range: 3-184 months). The pattern of failure was loco-regional in 66 (42.6%) and distant in 89 (57.4%) patients, respectively. Among patients with loco-regional failure, genitourinary and gynaecological cancers were the most prevalent primary tumours, each being diagnosed in 22 (33.3%) cases. Furthermore, the predominant site of relapse (47%) was the pelvic area. Only 26% of locoregional relapses occurred contra laterally, with 74% occurring at the margin of the treatment field, or at the successive nodal station or at any nodes of the ipsilateral chain (Fig. 1). The sites of treatment which more frequently showed recurrences in neighbouring (marginal and successive) lymph node areas were the abdomen and the pelvis (41%, for both). The median follow-up of the overall series was 68 months (range 10-324 months).
Conclusion
Relapses following SBRT/SRS nodal irradiation were somewhat more common in distant regions than in loco-regional sites in our study. The most common scenarios for locoregional relapse appear to be genitourinary or gynaecologic cancer and the pelvic site. Additionally, recurrences are not infrequent in the immediate surrounding lymph nodal sites.