Short course radiotherapy for advanced head and neck cancer: a phase 2 study
Nick West,
United Kingdom
PD-0066
Abstract
Short course radiotherapy for advanced head and neck cancer: a phase 2 study
Authors: Nick West1, Maha Zarroug1, Rahul Patil1, Joesf Kovarik1, Charles Kelly1, Malcolm Jackson1, Shahid Iqbal1
1Newcastle upon Tyne Hospitals Trust, Northern Centre for Cancer Care, Newcastle upon Tyne, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Incurable head and neck cancer has always proven difficult to manage. Patients ineligible for definitive, radical treatment are often offered palliative radiotherapy for disease and symptom control but for this cohort of patients, optimal dose fractionation remains unknown. Here we present highly conformal short course radiotherapy, 25 Gy in 5 fractions, delivered over 1 week. The objective being to evaluate whether there is opportunity to improve the therapeutic ratio for this challenging patient cohort, with comprehensive clinical follow-up and documenting progression free survival (PFS) and overall survival (OS).
Material and Methods
Patients from a single academic centre with advanced HNC, unsuitable for radical treatment were offered 25 Gy in 5 daily VMAT fractions over 1 week to the gross tumour volume.
Inclusion criteria
• Over 18 years of age
• Disease deemed incurable
• Declined definitive radical treatments
• Deemed unfit for definitive radical treatment
• Expected survival of >3months
Exclusion criteria
• Previous radiotherapy to the region
• Pregnant
Data was collected to enable survival and time to tumour progression calculations as well as record the toxicity. Patient and tumour baseline characteristics are summarised in table 1.
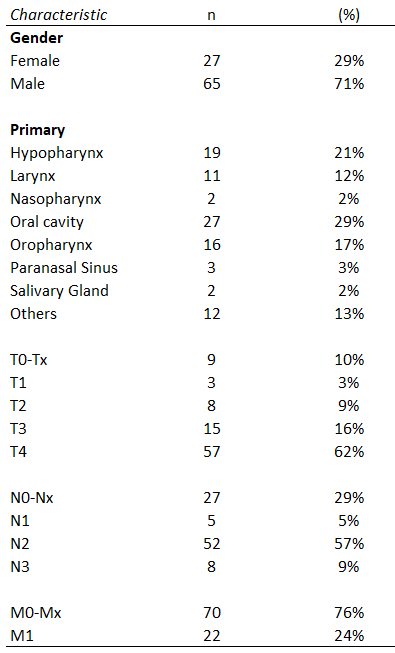
Table 1 Patient and tumour baseline characteristics
Results
Ninety-two patients (median age 71years; range 53-93years) were recruited and received the planned study dose (25Gy in 5 fractions). These patients were deemed unsuitable for radical radiotherapy because of extent of disease (59%), unfit for radical radiotherapy (35%) or the recurrence overlapped with previous radiotherapy (6%). Of these 73% had at least T4, N3, or M1 disease. Oral cavity was the most frequent subsite (29%), followed by hypopharynx (21%) and oropharynx (17%).
The median overall survival and progression free survival times were 7.9 and 7.5 months respectively with 1 and 2 year survivals of 38% and 18% (figure 1).
Treatments were well tolerated; no grade 4 or 5 toxicity observed and only 18% of patients demonstrating any grade 3 toxicity over the course of their follow-up.
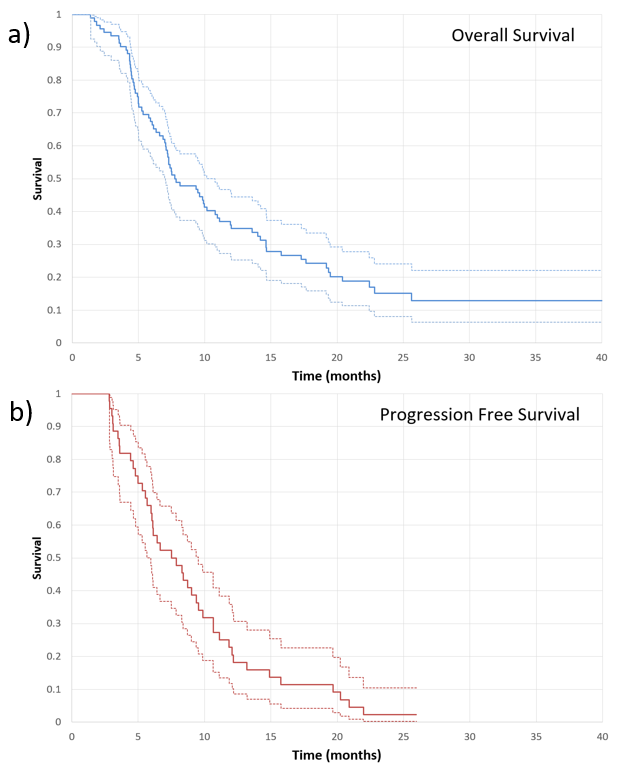
Figure 1 Survival curves, in months, from the time of radiotherapy with numbers at risk. a) Overall survival; median 7.9 months. b) Progression free survival; median 7.5 months.
Conclusion
This study, utilising hypofractionated radiotherapy (25Gy in 5 fractions), targeting the small volume macroscopic disease, utilising PTV margins appropriate for modern IGRT and VMAT techniques, has generated practice changing results commensurate with the literature. There were minimal side effects reported, suggesting this is a safe and feasible technique and further dose escalation should be investigated in prospective studies to achieve longer locoregional control.
We conclude that even frail patients with incurable head and neck cancer can benefit from a short course of highly conformal radiotherapy to the gross target volume to stabilise and decrease disease related symptoms.