Comparison of head-and-neck treatment plans on MR-Linac versus CBCT-Linac.
Roel Bouwmans,
The Netherlands
PD-0315
Abstract
Comparison of head-and-neck treatment plans on MR-Linac versus CBCT-Linac.
Authors: Roel Bouwmans1, Maartje Schoenmakers1, Niels Raaijmakers1, Mischa De Ridder1, Marielle Philippens1
1UMC Utrecht, Radiotherapy, Utrecht, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
In our clinical practice, palliative head and neck squamous cell carcinoma (HNSCC) patients are treated with a hypo-fractionated radiotherapy (6x6Gy). Patients are immobilized with thermoplastic mask and position verification is performed using a CBCT. Our aim is to compare the online adapted MR-Linac (Unity, Elekta) treatment with a CBCT-Linac treatment for HNSCC patients. The hypothesis is that the tumor volume will shrink during treatment, so with online adaptive treatment we can achieve a lower volume that receives high dose and therefore a lower organ at risk (OAR) dose.
Material and Methods
We performed a plan comparison (Monaco, Elekta) for 5 HNSCC patients who received an online adapted IMRT treatment of 6x6 Gy on the MR-Linac. We created a regular VMAT plan for each patient for the CBCT-Linac and re-calculated this plan on the daily MRI which were used to adjust the GTV delineation for the online MR-Linac treatment. The PTV margins were equal, except for fixed GTVs, that are reduced with 1mm on the MR-Linac. To assign electron densities the MR-image are segmented in bony structures, air cavities and the external body contour. We used this bulk-density CT of each fraction to re-calculate the VMAT plan to compare the DVHs with the structures created on the online MRI. The DVH comparison yields the daily treatment difference between plan parameters for the patients treated on the MR-Linac versus those when treated on the CBCT-Linac. The GTV volume change during treatment was measured. Average conformity index was calculated (total V95% / total PTV) and PTV coverage (V95%) was measured for all patients for both VMAT and IMRT plans. The average dose and the volume receiving 95% of prescribed dose was measured for all salivary glands close to the PTV.
Results
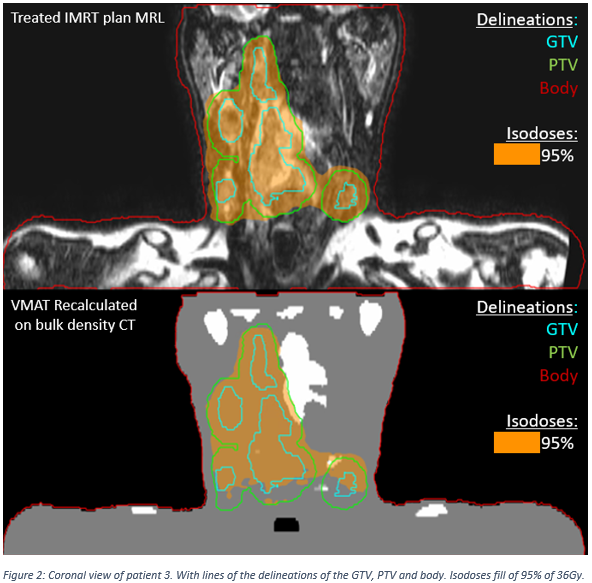
The GTV volume decreased during treatment for most patients with an average of all GTVs of 25.6%. (figure 1) The conformity index (CI) of the IMRT plans was the same for each fraction (range 1.2 – 1.4), while for the VMAT plans the CI was fluctuating (range 1.0 – 2.1). The PTV coverage for all MR-Linac treatments was acceptable (range 96.2% - 99.4%), but with VMAT there was an under dosage for some patients (range 85.3% - 96.4%). When a PTV is more caudally located we see a higher degree of under dosage, caused by a different shoulder position (figure 2). The mean dose of the salivary glands for VMAT was similar to IMRT. The relative volume of the salivary glands that receives high dose (V95% of 36Gy) was lower with IMRT (14%) than with VMAT (17%).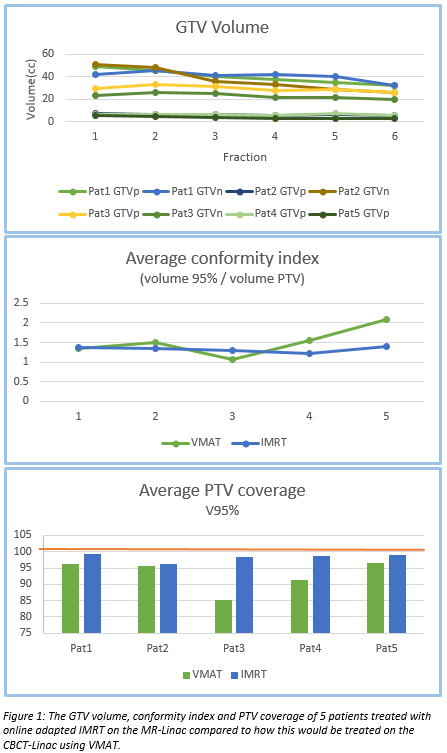
Conclusion
As hypothed, the PTV volume was decreasing, while the high dose region in relation to the actual PTV is stable for the IMRT-MR-Linac plan and fluctuating with the VMAT-CBCT plans. Although the high dose volume was high, the coverage of the VMAT plans was reduced to 85.3%. In the salivary glands, this resulted in a reduction of the volume receiving more than 95% prescribed dose of 3%, while the mean dose was similar.