Defining PTV margins for dose escalated, hypofractionated radiotherapy for rectal cancer.
Lynsey Devlin,
United Kingdom
PD-0314
Abstract
Defining PTV margins for dose escalated, hypofractionated radiotherapy for rectal cancer.
Authors: Lynsey Devlin1, Sean O'Cathail2, Gail Marshall1, Catherine Hanna3, Alice Paterson1, Aileen Duffton1
1Beatson West of Scotland Cancer Centre, Radiotherapy, Glasgow, United Kingdom; 2Institute of Cancer Sciences, University of Glasgow, Glasgow, United Kingdom; 3Beatson West of Scotland Cancer Centre, Clinical Oncology, Glasgow, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Dose escalated, hypofractionated radiotherapy for rectal cancer may be advantageous; due to the dose response relationship, moderate α/β ratio (∼5) of rectal cancer and the low radiobiological dose. Previous in-silico work has demonstrated this is feasible. The effect of set-up uncertainties and differential motion could be more of a concern when delivering a large dose per fraction. We aimed to determine the PTV margins required for dose escalation in short course radiotherapy of rectal cancer.
Material and Methods
Patients who had received 25Gy/5# were included, immobilised supine with a full bladder. Volume delineations were as per UK guidelines (RCR). Treatment PTV was created from ICTV + 7mm margin. Daily pre and post CBCT images were acquired, with all setup errors in 3 DoF corrected for.
Retrospective analyses of uncorrected error and motion were performed on CBCT datasets, using the below criteria.
To assess inter- and intra-fraction error, an automatic bony registration was performed with a defined ROI. Registrations were recorded for pre and post CBCT images for both 3 and 6 DoF. The difference of pre and post registrations were defined as intra-fraction error.
To assess inter- and intra-fraction soft tissue motion, iterative registrations were performed using GTV and ICTV. All structures were individually registered in anterior, posterior, superior, inferior, right and left translations. Required anisotropic PTV margins for GTV and ICTV were calculated using the Van herk et al. (2.5 Σ+0.7 σ) formula for a minimum dose coverage of 95% for 90% of patients i.e. PTV margin required for a SIB technique.
The maximum value for any direction was considered representative of the maximum structure inter- and intra-fraction motion.
Results
20 Rectal cancer patients were included. Patient median age was 70 (IQR 65-77), F (n=8), M (n=12). Rectum level was low (n=10), mid (n=5) and upper (n= 5). In total 100 Pre and 100 Post CBCT (n=200) images were analysed, with 3500 individual registrations performed.
For inter-fraction setup errors, the mean (SD) corrected errors were -0.23cm (0.21), 0.07cm (0.5), -0.01cm (0.48) for VRT, LNG and LAT. The mean uncorrected rotational errors were -0.3° (0.87), -0.05° (1.08), 0.46° (1.07) for pitch, roll and rotation respectively.
Intra-fraction set up errors were -0.04cm (0.06), -0.16cm (0.24), -0.04cm (0.12), 0.56° (1.4), 0.02° (0.79), 0.28° (1.09) for VRT, LNG, LAT, pitch, roll and rotation respectively.
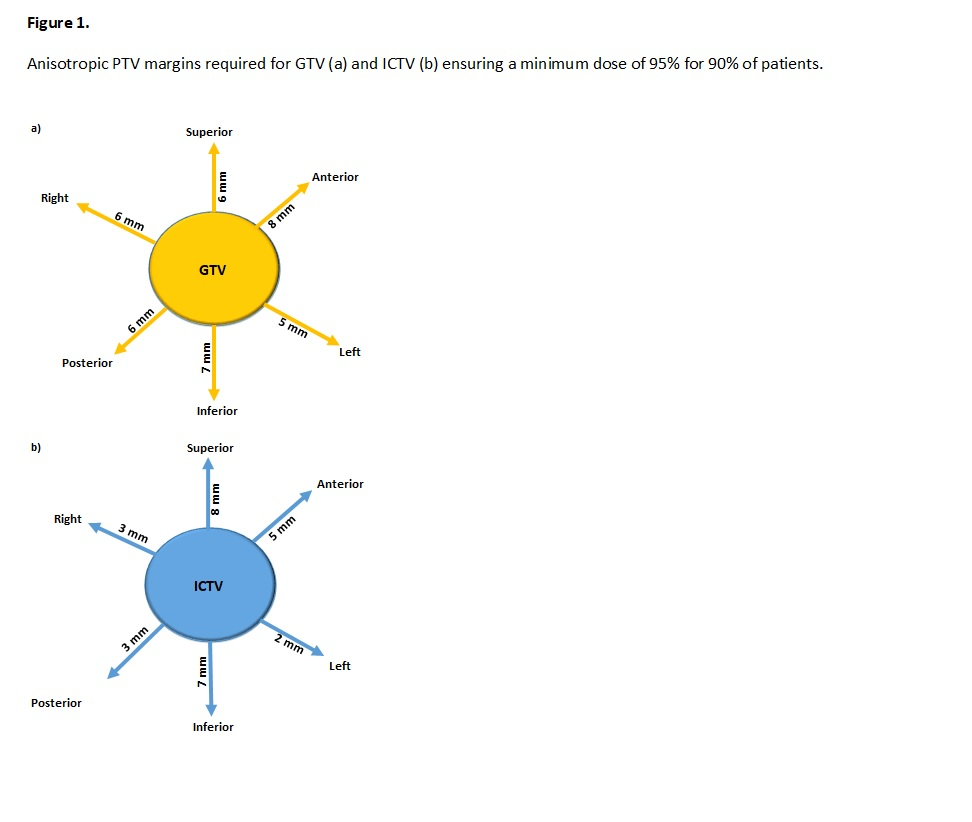
Uncorrected inter- and intra-fraction structure motions are reported in Table 1. The PTV margins required for 95% dose to the target for 90% of patients for GTV and ICTV are illustrated in Figure 1. 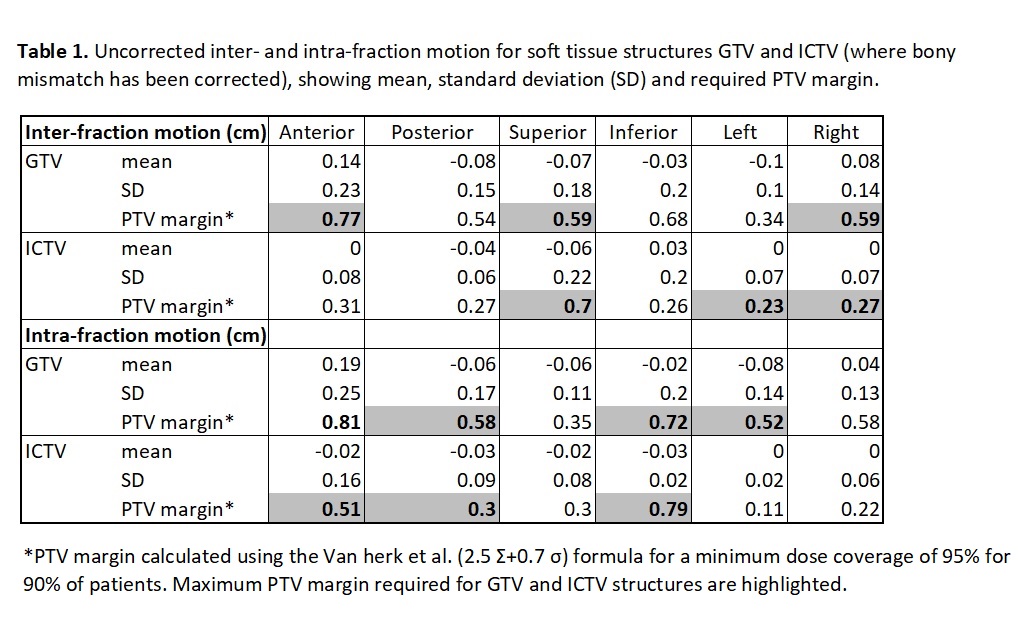
Conclusion
Matching to the extreme position of GTV and ICTV provides the maximum PTV margins required for dose escalated, hypofractionated radiotherapy for rectal cancer. This study highlights the need to minimise all sources of differential motion when preparing for dose escalation.