Time analysis of CBCT-guided online adaptive radiotherapy in Prostate cancer treatment workflow
PD-0313
Abstract
Time analysis of CBCT-guided online adaptive radiotherapy in Prostate cancer treatment workflow
Authors: Claudio Votta1, Althea Boschetti1, Michele Aquilano1, Francesco Catucci1, Andrea D'aviero1, Paolo Gaias1, Francesca Gruosso1, Martina Iezzi1, Marco Marras1, Sebastiano Menna1, Danila Piccari1, Elisa Pilloni1, Domenico Piro1, Francesco Preziosi1, Flaviovincenzo Quaranta1, Alessia Re1, Nadia Ulgheri1, Valeria Verusio2, Vincenzo Valentini3, Davide Cusumano1, Gian Carlo Mattiucci1
1Mater Olbia Hospital, Radiotherapy, Olbia, Italy; 2Università Cattolica del Sacro Cuore, Istituto di Radiologia, Roma, Italy; 3Fondazione Policlinico Universitario A. Gemelli IRCCS, Diagnostica per Immagini, Radioterapia Oncologica ed Ematologia, Roma, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Since August 2021, cone-beam computed tomography (CBCT) -guided online adaptive radiotherapy (oART) is one of our department's treatment options for prostate cancer patients. Different studies show that oART leads to significant dosimetric advantages, both in terms of target coverage and in terms of OAR’s dose sparing. However, the additional steps required for oART can significantly prolong the total treatment time and pose a challenge for day-to-day clinical implementation. This study aimed to evaluate the timing of oART compared to standard non-adaptive radiotherapy (non-ART) in prostate cancer treatment.
Material and Methods
A total of 36 prostate cancer patients were treated between August 2021 and September 2022, using Ethos therapy (Varian Medical Systems, Palo Alto, CA, US). All patients were treated with a dose of 67,5 Gy in 25 fractions to the prostate and seminal vesicles; for patients with nodal involvement, an additional total dose of 50Gy was given to the nodes using a simultaneous integrated boost. The total treatment session time (Ttot) was evaluated as the time elapsed from the patient's entry into the bunker to his exit. The time required for the following workflow steps was prospectively documented: patient entry and set-up(Ts), CBCT acquisition and matching (Tm), delivery and exit (Td). For the oART treatment sessions, the CBCT acquisition and contouring (Tc) and planning time (Tp) was also recorded.
Results
In total, 676 fractions were evaluated: oART were used in 223 (33%) treatment fraction. The mean Ttot for non-ART treatments was 0:12±0:04 (hh: mm). For oART treatments, the Ttot difference was statistically significant (p<0,05) between treatment plans with (oARTn) and without nodes (oARTp); in particular the mean Ttot for oARTp was 0:24±0:06 and the mean Ttot for oARTn was 0:30±0:06 (Figure 1). Time statistics of the different workflow steps are provided in Figure 2. In oART, we spent most of the time on contouring review and manual adjustments with a mean Tc of 0:12±0:04 for oARTn and 0:09±0:04 for oARTp.
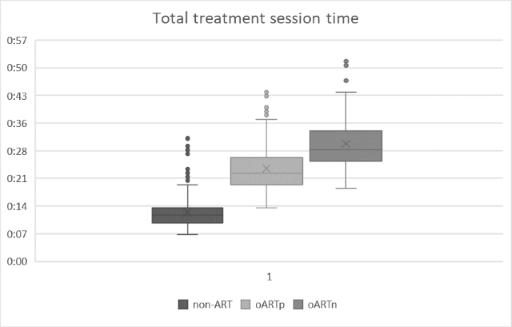
Figure 1. Box plot time distribution of Total treatment time
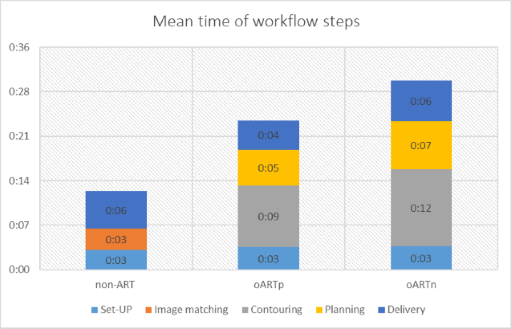
Figure 2 - Time distribution of non-ART and oART treatment workflow steps.
Conclusion
The time analysis carried out in this study suggests that CBCT- oART in prostate cancer may take more than twice as long as non-ART. In the future, improved AI segmentation and gaining more experience with the adaptive workflow may lead to achieving shorter oART treatments. Moreover, the relatively shorter treatment time may enable the large scale implementation of oART within a high-volume clinical practice.