Optimal use of limited proton resources for liver cancer patients
PO-1949
Abstract
Optimal use of limited proton resources for liver cancer patients
Authors: Louise Marc1, Jan Unkelbach1
1University Hospital Zurich, Radiation Oncology, Zurich, Switzerland
Show Affiliations
Hide Affiliations
Purpose or Objective
Objective: Liver cancer patients may benefit from proton therapy through isotoxic dose escalation. However, proton therapy is a limited resource and may not be available for all patients. We consider 5-fraction combined proton-photon liver SBRT treatments (CPPT), where only a subset of fractions is delivered with protons, and investigate how a limited number of proton slots is optimally used to maximize tumor control probability (TCP) in a patient cohort.
Material and Methods
Methods: Proton and photon plans delivering 10 Gy per fraction to the PTV were created for five liver cancer patients with PTV volumes varying between 348 cc and 641 cc. In CPPT, limited proton fractions may be optimally exploited by increasing the proton dose (i.e. upscaling the proton and downscaling the photon plan). To determine the proton and photon fraction dose, we maximize the BED_10^T to the PTV while constraining the mean normal liver (NL=Liver-GTV) BED_3^NL to the equivalent of 16 Gy mean NL dose (MLD) in 5 fractions. For patients where BED_10^T exceeds 150 Gy, we minimize the cumulative mean NL BED_3^NL while delivering a cumulative BED_10^T of 150 Gy. The resulting CPPT balances the benefits of fractionation in the NL versus exploiting the superior proton dose distributions. For each patient and each number of proton fractions, the resulting BED_10^T and the corresponding TCP [1] is calculated. Finally, the total TCP of the patient cohort is maximized by allocating the available proton slots to the patients who benefit the most of it.
Results
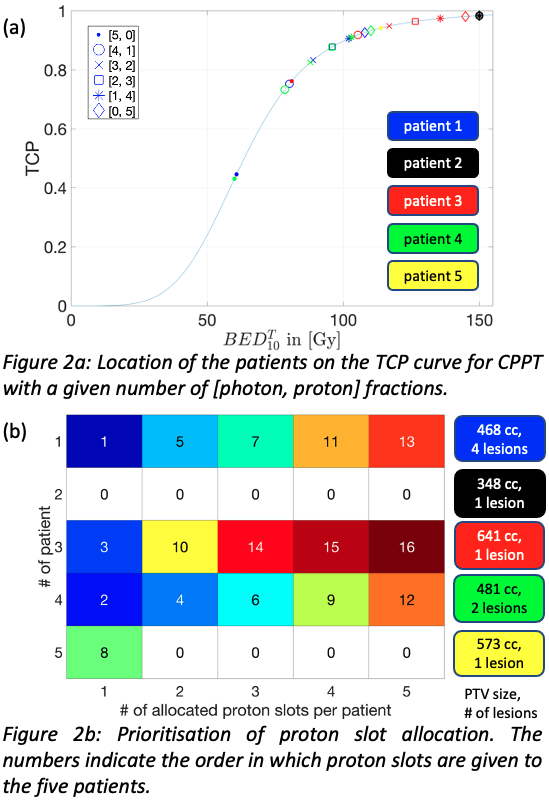
Results: For all patients considered, proton plans allowed for PTV dose escalation for a given maximum MLD. Figure 1 illustrates the increase in TCP with each additional proton fraction for patient 1. Compared to a photon treatment delivering 5x7.1 Gy to the PTV, a single proton fraction of 19.5 Gy and 4 photon fractions of 4 Gy yield a 30.7% TCP increase (from 44.6% to 75.3%) while delivering the same MLD. Treating patient 1 exclusively with protons yields an additional increase in TCP by 17.4% (to 92.7%). The benefit of an added proton slot varies from patient to patient and depends on both the location on the TCP curve and the dosimetric advantage of protons over photons (Figure 2a). Figure 2b illustrates how proton fractions are allocated by prioritizing patients with the highest benefit. For instance, if 11 out of 25 fractions are delivered with protons, patients 1/2/3/4/5 receive 4/0/2/4/1 proton fractions, which yield TCP increases of 46.1/0/18.7/47.9/4.2% compared to pure photon treatments. Thereby, all patients reach a TCP above 90%. With a sufficiently high number of available proton slots, the average TCP of the patient cohort can be increased by up to 24.9%.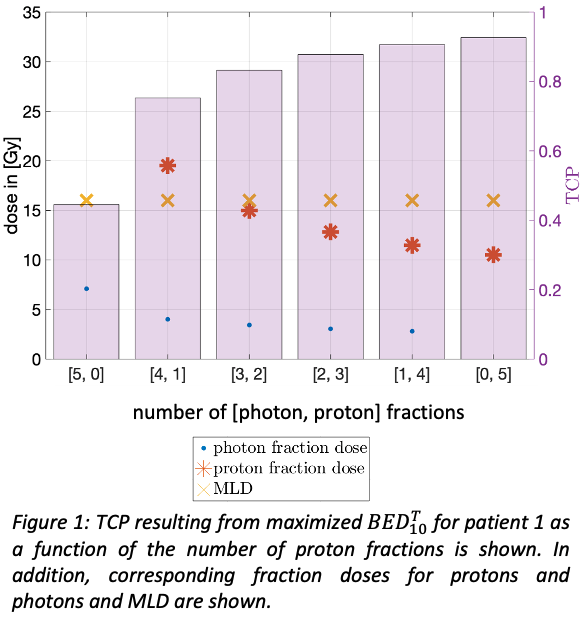
Conclusion
Conclusion: Limited proton resources can be optimally exploited via CPPT by increasing the PTV dose in proton fractions and allocating them to patients with the highest increase in TCP.
[1] A. Lausch et al., Br. J. Radiol., vol. 86, no. 1027, 2013, doi: 10.1259/bjr.20130147.