CBCT-guided online adaptive radiotherapy in patients with cervical cancer
Lisanne Zwart,
The Netherlands
PO-1424
Abstract
CBCT-guided online adaptive radiotherapy in patients with cervical cancer
Authors: Lisanne Zwart1, Siete Koch1, Laura Haverkate1, Ellen Hendriksen1, Eveline Koiter1, Judith Dasselaar1
1Medisch Spectrum Twente, Radiotherapy, Enschede, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
In image-guided radiotherapy (IGRT) of cervical cancer patients, an ITV is used to compensate for inter-fractional target motion. As a result, the PTV is relatively large, resulting in higher dose to the surrounding organs at risk (OARs). CBCT-guided online adaptive radiotherapy (oART) can be used to correct for inter-fractional motion and target volume differences on a daily basis, potentially resulting in less dose to the OARs. The aim of this study was to quantify the effect of oART for cervical cancer patients in terms of target coverage, OAR doses and PTVs.
Material and Methods
oART was simulated for five cervical cancer patients who were clinically treated in IGRT mode on a conventional linac. In addition, two cervical cancer patients were clinically treated with CBCT-guided oART using Ethos therapy (Varian Medical Systems, Palo Alto, CA, US) between March and October 2022. Each patient was treated in 25 fractions of 1.8 Gy. CTV-T-LR and CTV-E4500 (up to the aortic bifurcation) were contoured on the planning CT scan according to the Embrace protocol. A 9- or 12-field IMRT reference plan was created using a CTV-PTV margin of 5 mm in lateral and 8 mm in superior-inferior and anterior-posterior directions. oART was simulated and/or evaluated for five CBCTs per patient (one per week). During the adaptive workflow, OARs and CTVs were contoured and propagated and two treatment plans were created. The scheduled plan is the recalculated reference plan and the adapted plan is the re-optimized reference plan. For both plans, PTV coverage (V95%) and OAR doses (V40Gy of bladder, rectum and bowel bag) were evaluated. Moreover, PTV volume differences between planning CT and weekly CBCTs were analyzed.
Results
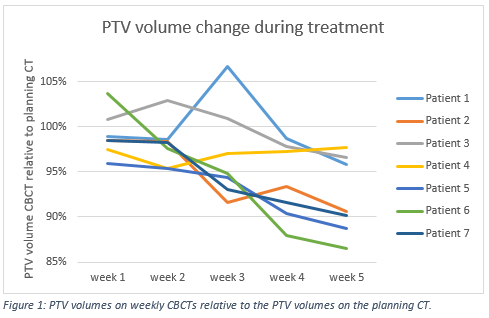
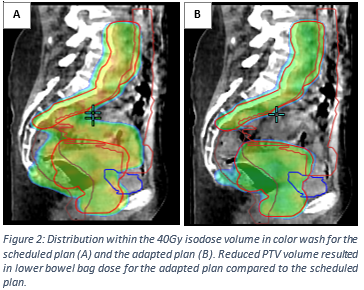
For all patients and analyzed fractions, PTV coverage increased for the adapted plan compared to the scheduled plan. Mean increase was 4.5±3.7% (range: 0.2-15.9%). In addition, mean difference of V40Gy of bladder, rectum and bowel bag was -3.4±9.9% (range: -23.0-13.5%), -3.4±15.1% (range: -23.8-37.9%) and -1.6%±4.0% (range: -10.1-4.9%), respectively for the adapted plan compared to the scheduled plan. For all patients, PTV volumes decreased gradually during treatment relative to the planning CT due to tumor shrinkage (Figure 1). Mean decrease of PTV volume for CBCT in the last week of treatment relative to the planning CT was 7.7±4.3% (range: 2.4-13.5%). PTV volume reductions were strongly correlated with bowel bag V40Gy decrease (Pearson’s R=0.76), see illustrative comparison in Figure 2.
Conclusion
oART resulted in increased target coverage, but not necessarily in less bladder and rectum dose as compared to the scheduled plans. Besides correction for position changes of the target, the main advantage of oART for cervical cancer patients was the possibility to correct for target volume reductions, that resulted in lower bowel bag doses.