The impact of 10MV FFF beams on delivery time for phase gated SBRT lung radiotherapy
Rafail Panagi,
United Kingdom
PO-1895
Abstract
The impact of 10MV FFF beams on delivery time for phase gated SBRT lung radiotherapy
Authors: Rafail Panagi1, Andrew Willett1, Robyn Stansbridge1
1The Clatterbridge Cancer Centre, Physics, Liverpool, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
SBRT for lung cancer can be performed under phase-gated conditions to reduce target motion. This allows for a smaller target volume, reducing dose to normal tissue (NT). However, as treatment then occurs for only a section of the breathing cycle, the treatment duration is extended, increasing the risk of clinically significant intra-fraction motion. Phase-gating may not be feasible for some hypo-fractionated treatments due to the relatively long treatment times associated with large doses per fraction, during which patients need to breathe reproducibly. It is hoped that the higher dose achievable with 10MV Flattening Filter Free (FFF) beams will reduce treatment times and allow the use of phase gating for all the locally implemented SBRT lung prescriptions. However, the effect might be diminished due to limitations such as gantry and MLC speed and MU required.
Material and Methods
To examine this, fifteen patients, five from each local protocol (54Gy/3#, 55Gy/5#, 60Gy/8#), were re-planned with 6FFF and 10FFF beams. The plan quality was assessed using the metrics; D99% to assess target coverage, D0.5%, Lung V20Gy, the Gradient Index (GI) and the Conformity Index (CI). Delivery accuracy was determined using ArcCHECKTM (Sun Nuclear), and treatment delivery time was measured for two duty-cycles, 30% and 50%.
Results
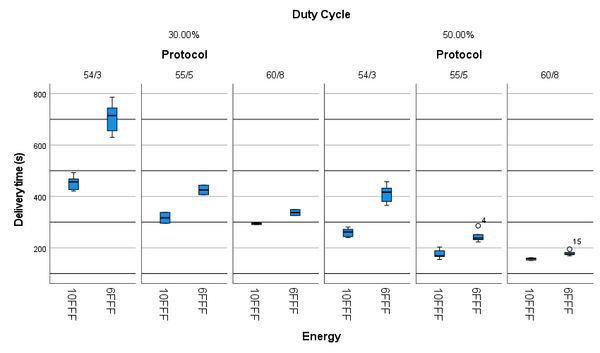
Time measurements indicated that treatment duration with 10FFF was faster compared to 6FFF for both duty-cycles and all protocols, see figure 1. The most significant reduction was observed for 10FFF 54Gy/3# plans, which were on average reduced by 2.5 minutes for the 50% duty-cycle (p < 0.001) and 4.2 minutes for the 30% duty-cycle (p < 0.001), and were similar in duration to the average 55Gy/5# 6FFF plans (p = 0.424 and p = 0.939, for the 50% and 30% duty-cycles respectively).
Plans produced with 6FFF beams were statistically superior to 10FFF in terms of GI, CI and Lungs - IGTV V20Gy, however, statistically significant difference may not translate to clinically significant difference. The impact of treatment reduction in intra-fractional motion and allowing hypo-fractionated prescriptions to be treated under phase-gated conditions may outweigh these differences. Planning was performed using the same Normal Tissue Objectives (NTO) for both energies. These are not optimised for 10FFF planning and may have contributed to the statistical inferiority. 10FFF plans required on average 2.18 more MU/Gy rendering them more complex, however, arcCHECKTM results showed that all plans passed the 95% gamma passing rate when assessed using a 3mm/3%, 20% threshold and global normalisation criteria.
Conclusion
All SABR lung patients are likely to benefit from delivery time reduction. Average beam-on times between 54Gy/3# 10FFF and 55Gy/5# 6FFF were within 10% for both the 50% and the 30% duty-cycles, hence, being comparable. This would possibly allow the delivery of the 54Gy/3# protocol under phase-gated conditions using 10FFF, which was not available with 6FFF due to extended treatment time.