Clinical implementation of ExacTrac Dynamic DIBH for left sided breast patients.
PO-1884
Abstract
Clinical implementation of ExacTrac Dynamic DIBH for left sided breast patients.
Authors: Thierry Gevaert1, Cristina Teixeira1, Jorn Ketelaers1, Adrian Gutiérrez2, Marlies Boussaer2, Anne-Sophie Bom2, Jelle Smeulders2, Thomas Mulliez2, Mark De Ridder2
1UZ Brussel, Vrije Universiteit Brussel, Radiotherapy, Brussels, Belgium; 2UZ Brussel, Vrije Universiteit Brussel, Radiotherapy, Radiotherapy, Brussels, Belgium
Show Affiliations
Hide Affiliations
Purpose or Objective
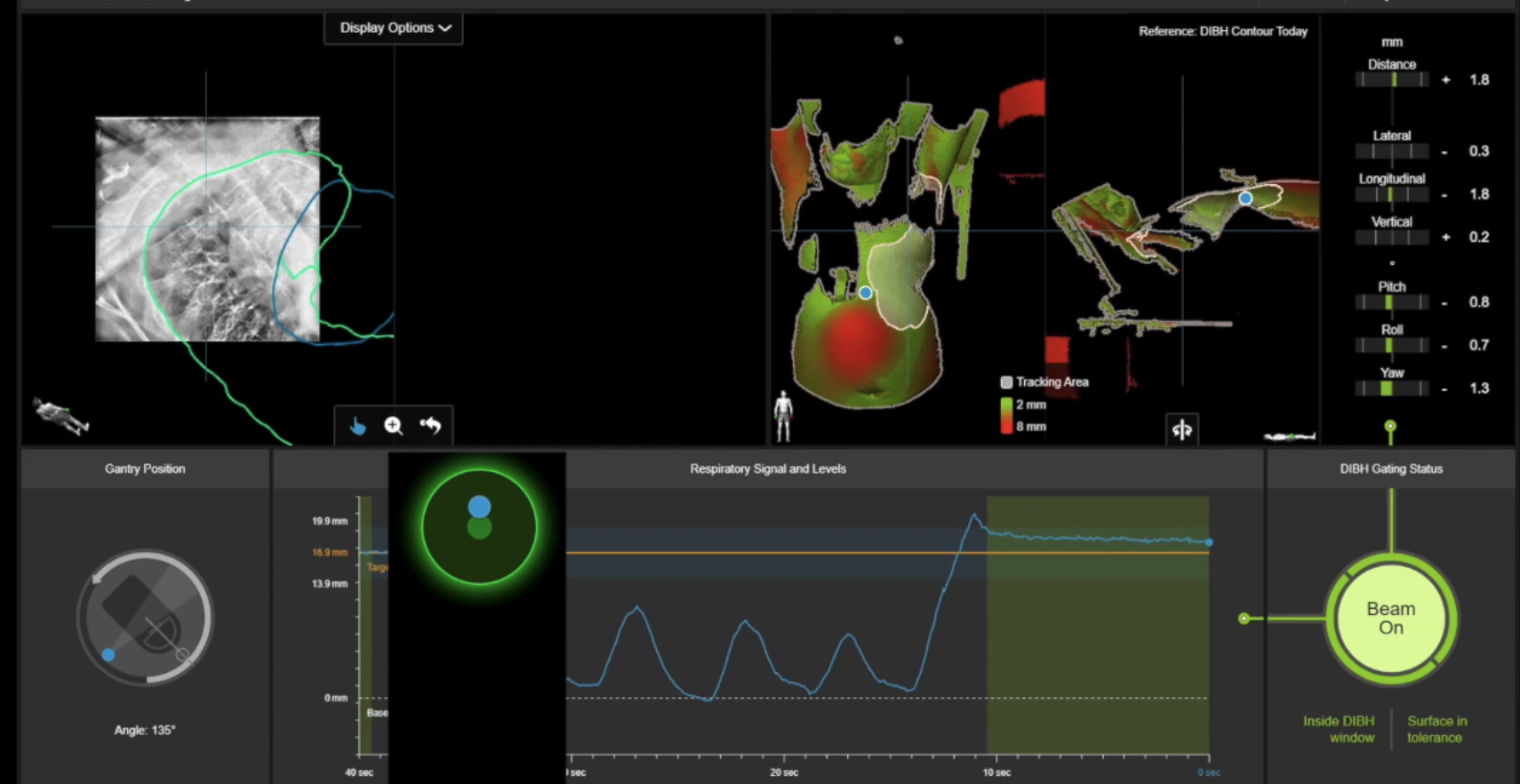
Left-sided breast cancer patients often receive deep inspiration breath-hold (DIBH) radiotherapy to reduce the relative risk of heart disease mortality. Recently ExacTrac Dynamic DIBH (Brainlab, Munchen, Germany) module was introduced into our department. This system combines surface-guided radiotherapy (SGRT) and image-guided RT for patient positioning, monitoring, breath hold control and tumor targeting. The purpose of this study was to validate this new workflow and to analyze intra-breath-hold stability and reproducibility in clinical practice.
Material and Methods
20 left sided breast patients treated with 40 Gy with a simultaneous integrated boost of 48 Gy in 15 fractions were included. Both a free- breathing (FB) and DIBH computed tomography (CT) at simulation was acquired and appropriate skin were delineated to quantify the rise of the surface due to DIBH. At the time of positioning, a region of interest was contoured on the surface in order to monitor intrafraction motion. A reference point was settled on the surface to generate the breathing signal. The system automatically generates the DIBH gating window based on the acquired FB and DIBH structure. Automated gating was performed using an audio-visual patient feedback system. Once patient is within the DIBH gate, stereoscopic x-rays are taken for positioning. This workflow was compared to our standard: RGSC (Varian, CA, USA) in combination with a gated CBCT. Patiens were positioned and gated for 7 consecutive fractions with our standard CBCT workflow and residual set up errors with stereoscopic x-rays were measured. For another 7 consecutive fractions, the new ExacTrac Dynamic workflow was used and residual set up analyzed with gated CBCT. Intra-breath-hold stability and reproducibility across all fractions of the entire treatment course were analyzed per patient.
Results
The mean residual set up errors when patients were positioned with a gated CBCT and verified with stereoscopic x-rays were 1.1mm (SD2.2mm), 0.1mm (SD3.1mm) and 0.5mm (SD3.1mm) for vertical, longitudinal, and lateral direction, respectively, and 0.2° (SD0.9°), 0.5° (SD1.5°) and 0.1° (SD1.4°), respectively, for yaw, pitch and roll. When residual set up of stereoscopic x-rays were analyzed based on gated CBCT, mean errors were 0.8mm (SD4.3mm), 0.4mm (SD3.3mm) and 0.2mm (SD3.6mm) for vertical, longitudinal, and lateral direction, respectively, and 0.2° (SD1.0°), 0.6° (SD1.4°) and 0.1° (SD1.6°), respectively, for yaw, pitch and roll. Average intra-breath-hold stability was 1.1mm (SD0.7mm) and 2.3mm (SD 1.3) for ExacTrac and RGSC, respectively.
Conclusion
This study demonstrated that stereoscopic x-rays are equally accurate as gated CBCT positioning for left sided breast DIBH treatments. Furthermore, x-ray imaging offers the possibility of evaluating the intra-DIBH stability to control the thoracical wall during irradiation.
The clinical integration of SGRT with IGRT with ExacTrac Dynamic enables a stable reproducible and reliable DIBH treatment delivery.