Gating strategy selection for patients with apical lung lesions in MRgRT SBRT
PO-1887
Abstract
Gating strategy selection for patients with apical lung lesions in MRgRT SBRT
Authors: Matteo Galetto1, Matteo Nardini2, Amedeo Capotosti2, Luca Boldrini3, Giuditta Chiloiro3, Angela Romano3, Claudio Votta3, Luca Indovina2, Lorenzo Placidi2
1Università Cattolica del Sacro Cuore, Facoltà di Medicina e Chirurgia, Roma, Italy; 2Fondazione Policlinico Universitario A. Gemelli IRCCS, UOSD Fisica Medica e Radioprotezione, Roma, Italy; 3Fondazione Policlinico Universitario A. Gemelli IRCCS, UOC Radioterapia Oncologica, Roma, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
greater patients’ compliance during free breathing (FB) respiratory motion management strategy has been observed, especially due to less treatment time and physical exhaustion (arms up) respect to deep inspiration breath hold (DIBH) strategy. The aim of this study is to quantify the GTV motion of apical lung lesions during a SBRT in a Magnetic Resonance (MR)-LINAC system, supporting the patient specific treatment gating pre-selection during the MR simulation procedure, by measuring the GTV centroid position on MR cine.
Material and Methods
12 patients with apical lung tumour treated with MRgRT SBRT at the ViewRay MRIDIAN system, have been retrospectively enrolled in this study. 6 of the 12 selected patients were treated in FB and the remaining 6 in DIBH gating technique. During the simulation and all the treatment fractions, sagittal cine 0.35T MR allows real-time GTV motion tracking. A home-made MATLAB script has been employed to perform image segmentation on MR cine for measuring the centroid position of the GTV contour. The GTV motion is evaluated by measuring the standard deviation of the GTV centroid position on all cine frames for FB patients, while for DIBH patients GTV motion was acquired during the deep inspiration phase (DIP) in simulation, first and last fractions cine, and when the patient breath freely in the simulation cine.
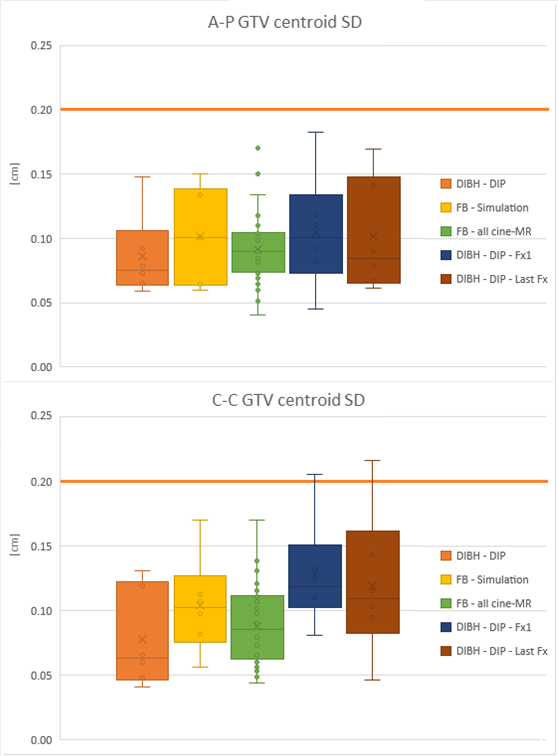
FB patients GTV motion was compared with the one measured in DIP for DIBH patients (Figure). Moreover, the position of 8 points on the GTV delineation and their relative motion have been calculated to verify the stability of the tracking algorithm. Homolateral lung and GTV volume have been also considered, together with maximum range of hepatic dome during the respiratory phase to further evaluate possible correlation with GTV motion.
Results
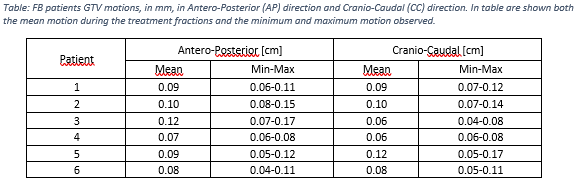
From ViewRay TPS 46 MR cine have been exported and a total of more than 8 hour and 29000 frames have been analyzed. GTV contour centroid shows a standard deviation of less than 2.2 mm in both directions during the DIP of DIBH patients. No differences due to patient training between the first and last fraction was observed (Figure). For FB patients, GTV motion ranges from 0.4 mm to 1.7 mm in the antero-posterior and cranio-caudal direction (Table); GTV motion during the treatment have been always in agreement with the one measured during the simulation (Figure). The analysis of the relative motion of the 8 points on the GTV shows that motion measurements are not affected by tracking algorithm. No correlations have been observed between GTV motion, lung and GTV volumes and hepatic dome excursion.
Conclusion
Simulation MR cine allows to select lung patients that can be treated in FB gating technique. When GTV contour centroid shows a standard deviation of less than 2mm, target motion will be the same as for a DIBH treatment. Future studies will investigate the dosimetric effect for margin reduction in FB patients, and motion in other lung districts.