Online adaption in short-course radiotherapy reduce bowel irradiation
Johanna Austrheim Hundvin,
Norway
PO-1867
Abstract
Online adaption in short-course radiotherapy reduce bowel irradiation
Authors: Johanna Austrheim Hundvin1,2, Unn Hege Lilleøren1, John Alfred Brennsæter1, Karoline Lewinsen2, Sara Pilskog1,2
1Haukeland University Hospital, Department of Oncology and Medical Physics, Bergen, Norway; 2University of Bergen, Department of Physics and Technology, Bergen, Norway
Show Affiliations
Hide Affiliations
Purpose or Objective
The RAPIDO trial in locally advanced rectal cancer (LARC), where short-course radiotherapy (RT) was followed by intensified chemotherapy, showed a reduction in distant metastases at the cost of an increased bowel toxicity. Cone beam CT (CBCT)-based online adaptive RT (ART) has potential to spare exposure of the adjacent healthy tissue, but requires knowledge on CTV-to-PTV margins to account for intra-fraction motion. As part of a clinical study, the goal of this study was therefore to explore margins robust to intra-fraction variation during online ART and quantify differences in dose to the bowel and bladder as compared to image-guided RT (IGRT).
Material and Methods
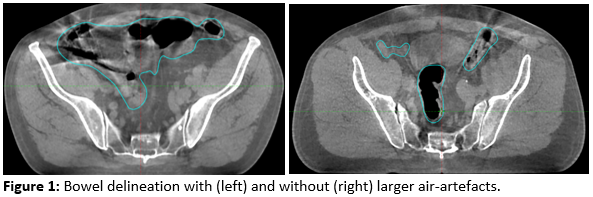
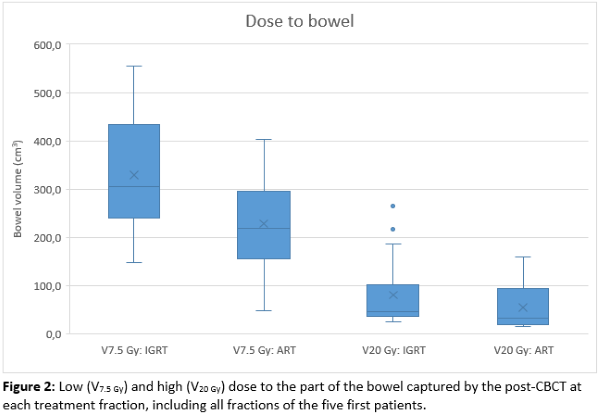
Prospectively enrolling 15 patients with LARC receiving pre-operative volumetric modulated arc therapy (VMAT) IGRT, both pre- and post-CBCT images from five treatment fractions per patient were acquired. The CTV, bowel loops and bladder were delineated on all images, with the exception of areas where air-artefacts forced the bowel loop contouring closer to a bowel bag structure, as seen in Figure 1. For IGRT, the ITV-to-PTV margins were 8 mm in all directions but ventrally where the expansion was 11 mm, according to clinical practice. For ART, the CTV was expanded with an isotropic PTV margin of 4 mm. Using the Ethos research software (the Emulator, Varian Medical systems, Inc.), online ART was simulated on the pre-CBCTs. Dose from the simulated IGRT and ART treatments were then overlaid on the six-degree bone-matched post-CBCT for dose evaluation in the Eclipse treatment planning system (Varian Medical systems, Inc.). The treatment was considered robust if average D99% to the CTV exceeded 95% on the post-CBCTs. The bowel volume receiving 7.5 Gy (V7.5 Gy ) and 20 Gy (V20 Gy) on the post-CBCTs were analysed, as both low and high dose levels can impact bowel toxicity. In addition, the mean dose to the bladder was analysed.
Results
Analysis of the five first patients show a CTV coverage of D99% ≥ 97% in all treatment fractions, thereby all adapted plans were considered robust based on our criteria. On average, the PTV volume was reduced by 28% compared to the IGRT PTV volume, resulting in a reduction in both low and high dose to bowel (Figure 2). Patients with larger PTVs tended to benefit the most from the adaption. The average bowel dose reduction in V7.5 Gy and V20 Gy were both 29%, while mean dose to bladder was reduced by on average 3%.
Conclusion
Robust online ART has the potential of sparing both low and high dose to the bowel, which is to be further verified on the rest of the cohort.