Real-time prostate and lymph node dose reconstruction accounting for independent 6DoF target motions
Karolina Klucznik,
Denmark
PO-1859
Abstract
Real-time prostate and lymph node dose reconstruction accounting for independent 6DoF target motions
Authors: Karolina Klucznik1, Thomas Ravkilde2, Simon Simon Skouboe1, Ditte Møller2, Steffen Hokland2, Paul Keall3, Simon Buus2, Lise Bentzen4, Per Poulsen5
1Aarhus University Hospital, Danish Center for Particle Therapy, Aarhus, Denmark; 2Aarhus University Hospital, Department of Oncology, Aarhus, Denmark; 3University of Sydney, ACRF Image X Institute,, Sydney, Australia; 4Department of Oncology, Aarhus University Hospital, Aarhus, Denmark; 5Aarhus University Hospital, Danish Center for Particle , Aarhus, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
High-risk prostate cancer patients require irradiation of both prostate and pelvic lymph nodes (LN) which undergo independent inter- and intrafraction motion composed of translations and rotations (six degrees of freedom, 6DoF). The dosimetric consequence of these motions have not been fully investigated. This study develops a method for real-time 6DoF motion-including dose reconstruction for two independently moving targets and applies it to investigate the actually delivered target doses for prostate patients.
Material and Methods
The study includes 5 patients treated in 39 fractions with 78 Gy to prostate CTV and 56 Gy to LN CTV using 3-arc VMAT. The CTV-to-PTV margins were 7-9 mm (prostate) and 5-8 mm (LN). A CBCT matched on three implanted prostate markers was used for setup. Triggered kV images acquired every 3 s during treatment delivery at ten fractions per patient were used for post-treatment estimation of the time-resolved 6DoF prostate motion during treatment using the formalism of kilovoltage intrafraction monitoring (KIM) to estimate the 3D motion trajectory of each marker. A 6DoF match of a post-treatment CBCT to the planning CBCT was used to estimate the 6DoF position of the LN assuming no intrafraction motion. Real-time motion-including dose reconstruction was performed post-treatment by sending data streams with machine parameters and the prostate and LN 6DoF motion to in-house developed software (DoseTracker) that calculated the 6DoF motion-including target doses by a simplified pencil beam algorithm. The motion-induced change in minimum dose to 95% of the prostate and LN CTVs (ΔD95%) was calculated for each fraction and for all investigated fractions averaged (planned and reconstructed dose were calculated by DoseTracker).
Results
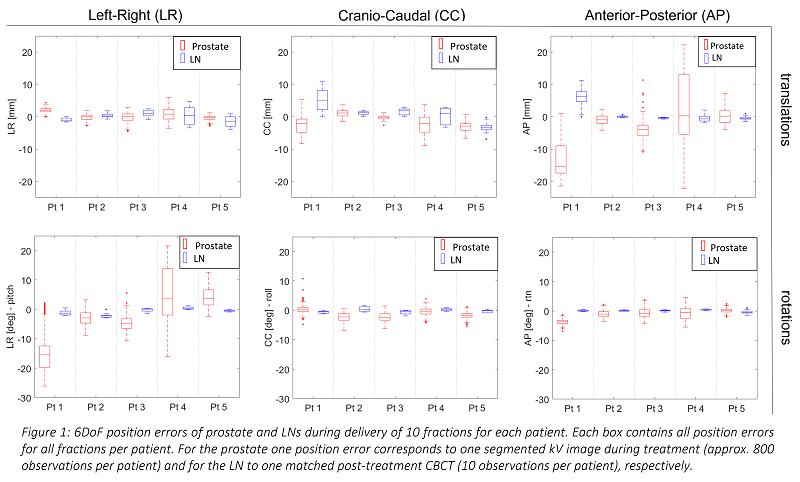
The largest observed 6DoF target position error (averaged over one treatment field) was 4.3 mm (LR), -6.7 mm (CC), -18.2 mm (AP) and -20.6° (LR), -2.7° (CC), -3.8° (AP) for prostate and 4.8 mm (LR), 10.9 mm (CC), 11.2 mm (AP) and 2.9° (LR), 2.1° (CC), 0.7° (AP) for LNs (see details in Fig 1). The largest observed intrafraction motion range occurring during one fraction was 5.1 mm (LR), 8.6 mm (CC), 18.5 mm (AP), 16.1° (LR), 13.9° (CC), and 5.2° (AP).
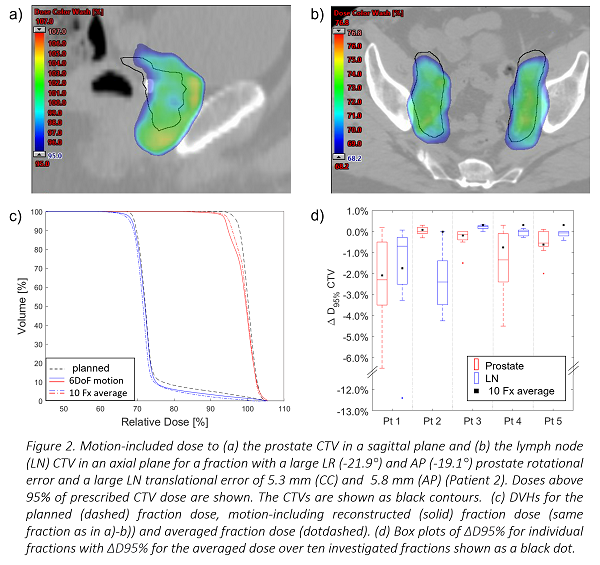
For a single fraction the CTV ΔD95% range was [+0.3;-6.5]% for prostate and [+0.3;-12.4]% for LN, illustrating considerable motion-induced reduction in CTV dose coverage at certain fractions (Fig 2). For the averaged dose over all the fractions the CTV ΔD95% range decreased to [+0.1;2.1]% for prostate and [+0.3;-1.8]% for LN (Fig 2d).
Conclusion
Triggered kV-images during treatment together with post-treatment CBTCs were successfully used to estimate the independent 6DoF prostate and LN motion. Motion-including dose reconstruction revealed large dose distortions for both targets at individual fractions which tended to smear out after more fractions. Nevertheless, the large ΔD95% for prostate observed for individual fractions can be important for stereotactic prostate treatments with less fractions.