Differences in coverage of GTV and PTV during the ten respiratory phases in SBRT of 50 lung tumors
Thomas Leth Fink,
Denmark
PO-2039
Abstract
Differences in coverage of GTV and PTV during the ten respiratory phases in SBRT of 50 lung tumors
Authors: Thomas Leth Fink1,2, Charlotte Kristiansen1, Torben Schjødt Hansen1, Torben Frøstrup Hansen1,2, Rune Slot Thing1
1Department of Oncology, Lillebaelt Hospital, University Hospital of Southern Denmark, Vejle, Denmark; 2Institute for Regional Health Research, University of Southern Denmark, Vejle, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
When planning stereotactic body radiation therapy (SBRT) of lung tumors, different approaches regarding dose prescription and reporting are in use throughout the world. We report the dose to GTV and PTV during each of the ten respiratory phases of the 4DCT treatment-planning scan for 50 patients treated with 66 Gy in three fraction SBRT prescribed to GTV.
Material and Methods
We retrospectively recalculated and analyzed the treatment plans on all 10 respiratory phases for 50 patients treated between 01-09-2021 and 01-09-2022. A dose of 66 Gy in three fractions was prescribed to the GTV with the aim of reaching GTV D95% = 62.7 Gy (if not possible due to adjacent OARs, GTV D99.9% = 42.75 Gy was accepted). For the PTV we aimed for PTV D98% = 45 Gy (if not possible due to adjacent OARs, PTV D98% = 30 Gy was accepted). For tumors located near the thoracic wall, risk adapted treatment planning ensured that the thoracic wall did not receive more than 45 Gy (aiming for D0.05cm3 < 35 Gy). We have no limitations for the maximum dose inside the GTV. A GTV is contoured on all 10 phases and summed to an ITV before adding a 5mm isotropic margin to create a PTV. The SBRT treatment is delivered as VMAT on Elekta linacs equipped with the Agility MLC, using a 10 MV FFF beam. Treatment planning is performed on the mid-position CT in RayStation 11B with two partial arcs delivering dose through the diseased lung only. 4D-CBCT imaging is performed before the first arc is delivered and repeated mid-fraction, with soft tissue match on the PTV.
Results
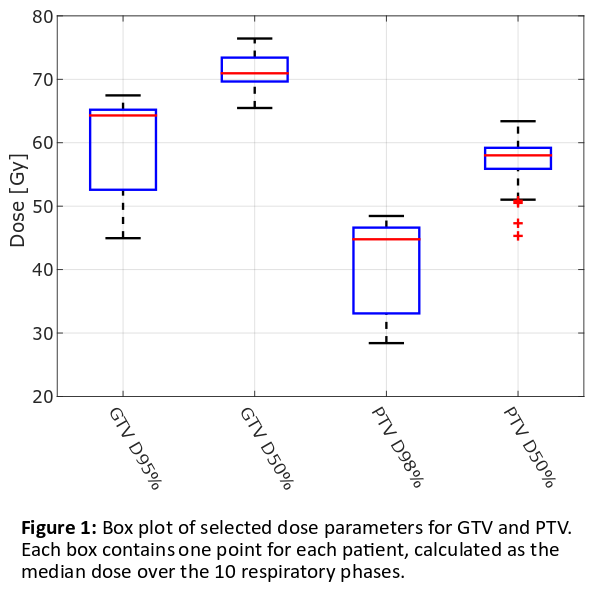
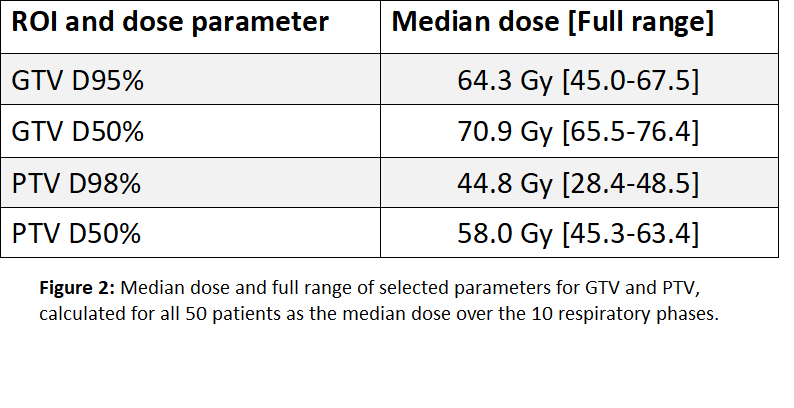
The median GTV D50% is 70.9 Gy and D95% is 64.3 Gy across all respiratory phases for all patients, which is higher than the aimed dose of 62.7 Gy (Figure 1 and 2). Nineteen out of the 50 patients had a median GTV D95% < 62.7 Gy due to tapering off the dose near the thoracic wall. The median PTV D50% is 58.0 Gy and D98% is 44.8 Gy across all patients, which is very close to the aimed dose of 45 Gy. Half the patients had a median PTV D98% < 45 Gy, also owing to the before-mentioned tapering off. The GTV motion was estimated to 0.64 cm in median, with a full range of 0.12-1.4 cm.
Conclusion
Our treatment approach ensures a high median dose to the GTV even when the tumor is located close to the thoracic wall. We believe this approach can deliver higher GTV doses compared to only prescribing a dose to the PTV, when dose escalation to the GTV is actively pursued even for tumors close to the thoracic wall. Even though we are planning on the mid-position CT, we show delivery of a high dose on all phases, confirming that this approach is robust with respect to respiratory motion. We believe that this practice of prescribing a dose for the GTV, but ensuring that demands are met for both GTV and PTV, is a relevant and reproducible strategy to use.