Benchmarking of a clinical proton pencil beam scanning model in GATE, Eclipse and RayStation
Daniela Botnariuc,
United Kingdom
MO-0482
Abstract
Benchmarking of a clinical proton pencil beam scanning model in GATE, Eclipse and RayStation
Authors: Daniela Botnariuc1,2, Steven Court3, Ana Lourenco1,2, Valerios Politidis1, Gary Royle1, Andrew Gosling3, Vasilis Rompokos3, Mohammad Hussein2, Catarina Veiga1
1University College London, Medical Physics and Biomedical Engineering, London, United Kingdom; 2National Physical Laboratory, Metrology for Medical Physics Centre, Teddington, United Kingdom; 3University College London Hospitals NHS Foundation Trust, Radiotherapy Physics Services, London, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Monte Carlo (MC) is becoming increasingly used in clinical proton therapy (PT) facilities for independent dose calculations. In this work, we developed and benchmarked a MC model of a clinical pencil beam scanning (PBS-PT) system and compared its performance with beam models built within commercial treatment planning systems (TPS).
Material and Methods
Four implementations of the beam model of a clinical PBS-PT system (Varian ProBeam) were investigated: one in GATE (v8.2) and three from two commercial TPSs - Eclipse proton convolution superposition algorithm (v16.1, Varian Medical Systems) and RayStation PB and MC (RaySPB and RaySMC) algorithms (v12.0.100.0, RaySearch Laboratories). The commissioning beam data consisted of integral depth dose (IDD) curves in water and profiles in air (nominal energies: 70–245 MeV) and was imported into both TPSs to create the beam models. In GATE, the beam model was implemented by iteratively tuning the beam parameters at the source to match the commissioning data. Range shifters (RS) were modelled from experimental profiles in air (Eclipse) or by modelling the material to match measured water equivalent thickness (RayStation/GATE). All models were first compared against the commissioning data, and then assessed in a set of box fields delivered to water. IDDs and lateral profiles in the centre of the volumes were compared for three 10×10×10 cm3 plans of spread-out Bragg peaks (SOBP) of 15, 20 and 30 cm range without a RS, and three 5×5×5 cm3 plans with RS of varying thickness (2, 3 and 5 cm). Additionally, the dose at the centre was measured for 19 box field plans with varying SOBP range (10 cm to 35 cm) and width (2 cm to 20 cm), covering a representative range of clinical energies.
Results
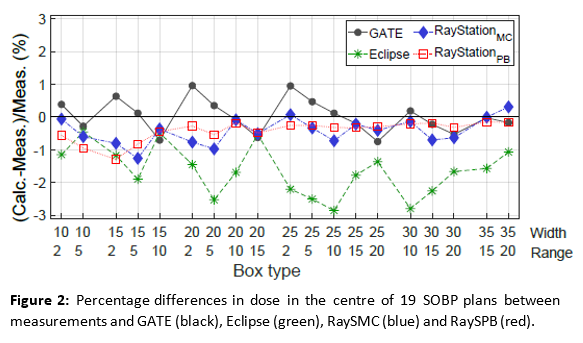
The differences in proton range (R80%) were within 0.4 mm for GATE and 0.1 mm for the TPSs, for all nominal energies. The absolute differences in Bragg peak width (W80%) were within 0.7 mm, with a trend for GATE and RayStation to overestimate W80%. The mean differences in spot size for x and y profiles were within 0.1 mm, for all planes. IDDs and lateral profiles for the 10×10×10 cm3 plan with 20 cm range (fig.1 (a) and (b)) presented good agreement; similar findings were found for plans with 15 and 30 cm range. IDDs for the 5×5×5 cm3 plan with RS=5 cm (fig.1 (c)) were within 5% for GATE, Eclipse and RaySMC, with RaySPB showing the largest differences. For the corresponding lateral profiles (fig.1 (d)), absolute differences within 7% were observed. Overall, smaller differences in IDDS and lateral profiles were achieved for plans with the remaining RSs. Differences in dose in the centre of SOBP plans with varying ranges and widths (fig.2) was within 3% for all algorithms, with Eclipse underestimating the dose for all cases.

Conclusion
The performance of the four PBS-PT models was benchmarked against experimental data. GATE provided an accurate independent dose calculation tool to support the commissioning and quality assurance workflows of clinical proton facilities.