Benefits of bespoke PTV margins for bladder cancer using CBCT-guided online adaptive radiotherapy
Rachel Hollingdale,
United Kingdom
MO-0882
Abstract
Benefits of bespoke PTV margins for bladder cancer using CBCT-guided online adaptive radiotherapy
Authors: Matthew Bolt1, Charlotte Shelley2, Rachel Hollingdale1, Chee Goh2, Elizabeth Adams1
1Royal Surrey Hospital NHS Foundation Trust, Radiotherapy Physics, Guildford, United Kingdom; 2Royal Surrey Hospital NHS Foundation Trust, Oncology, Guildford, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Online adaptive radiotherapy (oART) opens up the possibility of using bespoke PTV margins for each patient based on intra-fraction changes rather than inter-fraction based population margins. This should allow reduction in the volume of healthy tissue irradiated and in turn reduce treatment-associated toxicities.
We have conducted a planning study to assess the potential benefits of bespoke PTV margins based on the method outlined by Astrom [1]. This study assesses the feasibility of deriving bespoke margins based on the CBCT data from the first three treatment fractions and quantifies the potential dosimetric benefits compared with current local practice for patients having whole bladder radiotherapy.
Material and Methods
Retrospective measurements of the shift in target contours between CBCT1 and CBCT2 were recorded in the 6 orthogonal directions for each of the 188 oART fractions delivered to 10 oART bladder patients treated with 55Gy/20#.
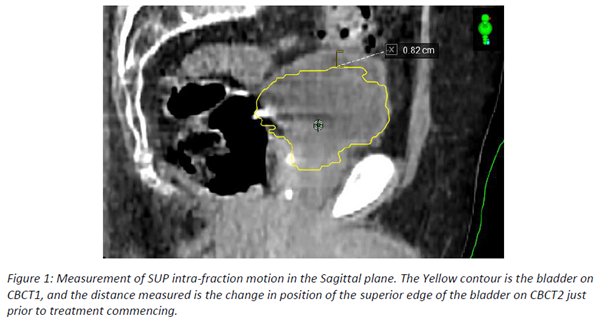
As part of the oART workflow on Ethos an initial CBCT (CBCT1) is taken. Using this, organs and targets are contoured and an adapted plan generated and compared to the original plan. Following plan selection a second CBCT is taken (CBCT2) and rigidly matched to the first to ensure target coverage is maintained prior to commencing treatment. The contours from CBCT1 are visibly overlaid on CBCT2 within the system allowing measurement of the intra-fraction changes as shown in Figure 1.
Bespoke margins for each patient were derived using the maximum measurement from the first 3 fractions in each direction plus an additional 5mm. Bespoke margins were evaluated on all remaining fractions to determine whether they would fully encompass the target in all cases.
Two 9-field IMRT plans were generated for full fractionation for each patient using the local planning template; one using standard margins, one with the bespoke margins. The original and bespoke PTV volumes were compared. Dosimetric values listed within the clinical protocol for the bowel (V39Gy, V43Gy, V48Gy, V52Gy) and rectum (V43Gy, V52Gy) were compared between the two plans.
Results
PTV volume reduced for all patients using bespoke margins; mean 17% (range 2% to 34%). Only 4 of 1128 measurements exceeded the bespoke margin threshold after fraction 3, all by less than 1mm.
No significant change in planned dose was found for the rectum.
Bowel dose reduced for 8 of 10 patients. V39Gy, V43Gy, V48Gy, and V52Gy reduced by a mean of 20%, 23%, 26%, and 31% respectively. The range of change in dose is shown in Figure 2.

Conclusion
Generation of bespoke margins for oART is feasible using the Varian Ethos and this study indicates that significant reductions in the PTV volume and bowel dose would result for a large proportion of patients.
The clinical workflow for routine implementation within a busy centre is under development, including collection of patient outcomes to assess patient benefit.
[1] Astrom. L. M. et al. (2022) Radiotherapy and Oncology Vol. 171, pp 37-42.