Prediction of radiation-induced taste loss with taste bud bearing tongue mucosa in HNC patients
Hendrike Neh,
The Netherlands
MO-0055
Abstract
Prediction of radiation-induced taste loss with taste bud bearing tongue mucosa in HNC patients
Authors: Hendrike Neh1, Suzanne P.M. de Vette1, Hung Chu1, Nanna M. Sijtsema1, Peter M.A. van Ooijen1, Roel J.H.M. Steenbakkers1, Johannes A. Langendijk1, Lisanne V. van Dijk1
1University Medical Center Groningen, Radiotherapy, Groningen, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Taste loss is a common yet complex toxicity of head and neck cancer (HNC) radiotherapy treatment. Prediction prior to treatment is important to minimize taste loss and maintain quality of life of HNC survivors. Radiation-induced toxicities are commonly predicted by normal tissue complication probability (NTCP) models. Taste NTCP prediction is based on the dose to the oral cavity. Stieb et al. (2021) proposed the taste bud bearing tongue mucosa as a new taste loss predictor. This project aimed to test the prediction of taste loss at 6 months after HNC radiotherapy with auto-segmented tongue mucosa compared to full oral cavity as identified in previously developed NTCP models.
Material and Methods
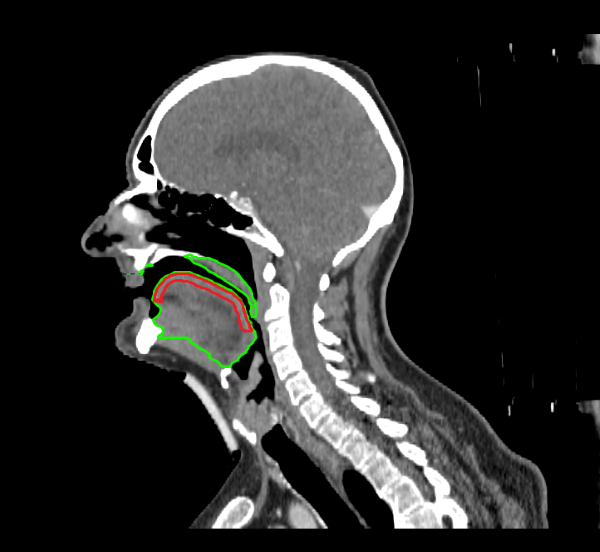
Included HNC patients were treated with curative radiotherapy between 2007 and 2022. The endpoint was patient-rated moderate-to-severe taste loss scored with the EORTC QLQ-H&N35. The previously published reference NTCP model included the oral cavity mean dose, combined parotid gland mean dose and age (Bosch et al. 2021). The new tongue mucosa structure was derived from the existing oral cavity structure by 1) creating an inner rim of 5 mm of the oral cavity structure and 2) trimming the posterior, anterior and inferior regions in accordance with Stieb et al. guidelines (see Figure). The performance of the mean dose admitted to this new structure was compared to the full oral cavity with both univariable analysis and a refit of the reference NTCP model substituting the tongue mucosa for the oral cavity structure.
Figure 1: Centred sagittal view of a CT with oral cavity structure delineated in green and auto-segmented taste bud bearing tongue mucosa structure delineated in red.
Results
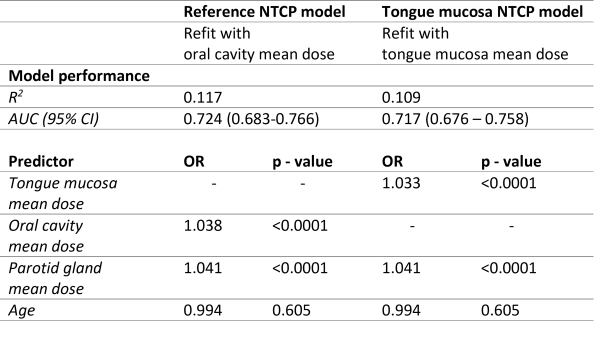
In total 434 HNC patients were included, of which 26.5% (n = 115) reported moderate-severe taste loss at 6 months post treatment. Visual inspection showed good conformity between the auto-segmented structures and the Stieb et al. guidelines. The mean dose to the full oral cavity was 31.0 Gy [IQR: 13.7 – 50.5] and for the tongue structure 27.3 Gy [IQR: 7.5 – 48.0]. The full oral cavity mean dose (OR=1.037; p=<0.0001) and combined parotid gland mean dose (OR=1.041; p=<0.0001) showed a larger dose response relation compared to the tongue mucosa (OR=1.031; p=<0.0001). The multivariable NTCP model showed similar results, as a model with the tongue mucosa mean dose (AUC: 0.724 95%CI [0.674-0.777]; R2=0.165) did not perform better than the reference model with oral cavity mean dose (AUC: 0.729; 95%CI [0.678 - 0.7802]; R2=0.178).
Table 1: Comparison of the NTCP model performance with oral cavity mean dose and the auto-segmented taste bud bearing tongue mucosa mean dose.
Conclusion
The taste bud bearing tongue mucosa structure did not outperform the oral cavity structure in the logistic regression NTCP model predicting late taste toxicity at 6 months. This might related to the limited mean dose differences between the both structures. This further underlines the complexity of predicting taste loss in HNC patients.