Reduction of the CTV margin in glioblastoma leads to dosimetric benefit without compromising outcome
MO-0556
Abstract
Reduction of the CTV margin in glioblastoma leads to dosimetric benefit without compromising outcome
Authors: Dario Di Perri1, Dianne Hartgerink2, Karin Terhaag2, Ruud Houben2, Inge Compter2, Daniëlle Eekers2
1Cliniques universitaires Saint-Luc, Radiation oncology, Brussels, Belgium; 2Maastricht University Medical Centre+, Radiation Oncology (Maastro), Maastricht, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Glioblastoma (GBM) is widely treated using large radiotherapy (RT) treatment margins (i.e., 2-3 cm around the surgical cavity/residual tumour) based on the fact that most GBM (i.e., ≥ 80%) recur within this area. Current ESTRO guidelines (Niyazi et al. 2016) advocate for a 20mm clinical target volume (CTV) expansion. However, accumulating data point towards a dose-dependent atrophy of cerebral structures after RT (Raschke et al. 2022; Nagtegaal et al. 2022), presumably associated with toxicity (e.g. cognitive decline). In this context, the question arises whether treatment volumes could be reduced. In 2018, the Dutch guidelines for GBM delineation were modified: CTV isotropic expansion was reduced from 20mm to 15mm (FLAIR hypersignal being still included within 20 mm around the GTV). We retrospectively analysed the impact of margin reduction on treatment volumes, dosimetric parameters for organs at risk (OARs), and patient outcome.
Material and Methods
All adult patients with GBM treated between 01-2015 and 12-2020 with concurrent chemoRT (60Gy/2Gy or 59.4Gy/1.8Gy) with temozolomide were analysed (n=124). Patients treated with a CTV margin other than 20 or 15mm (n=5) or who did not complete RT (n=6) were excluded. Of the 113 remaining patients, 57 were treated using a 20mm CTV margin (CTV20), and 56 with a 15mm margin (CTV15). Both patient groups were compared for target volumes (i.e., GTV, CTV, PTV), OARs dose parameters (i.e. brain, hippocampi, brainstem, optic nerves, chiasm, cochleas, and pituitary gland), progression-free survival (PFS), and overall survival (OS)).
Results
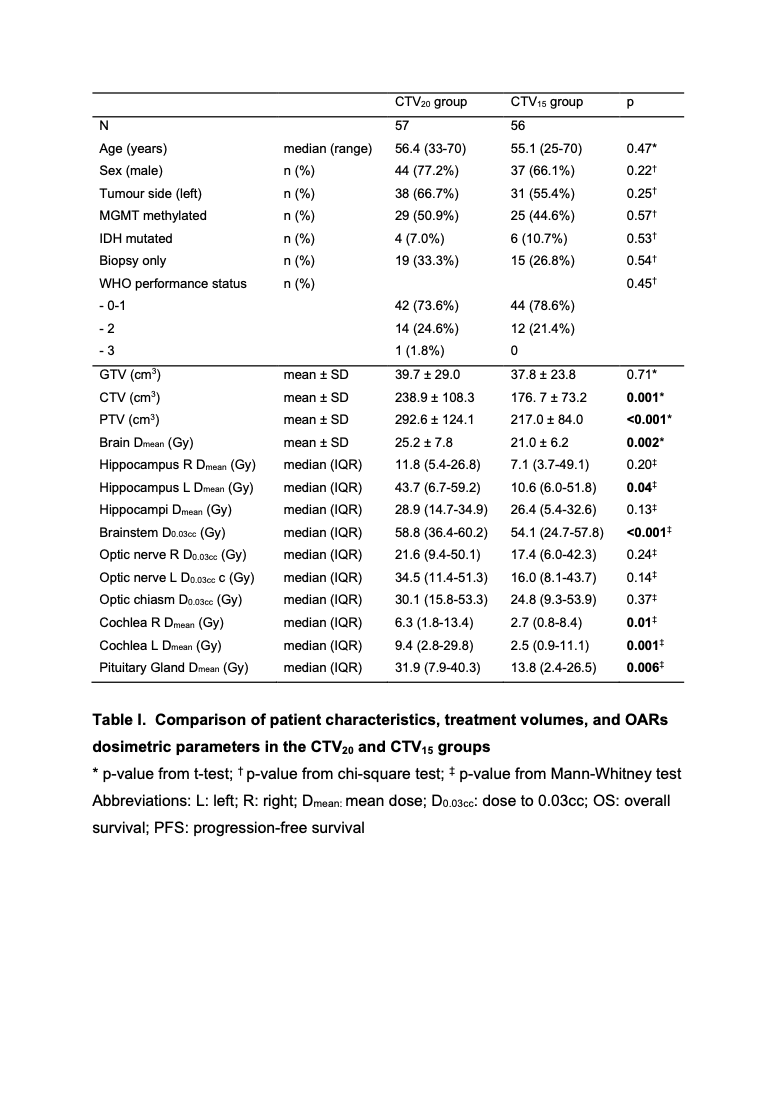
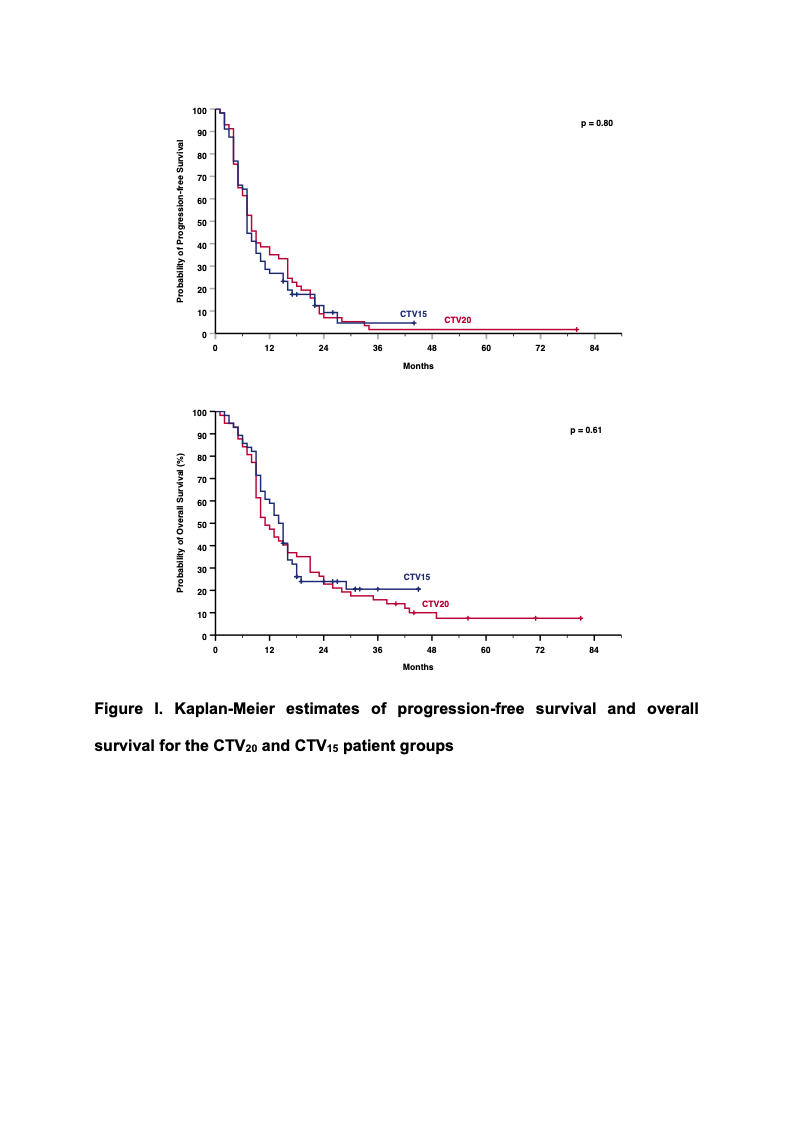
Patient characteristics are described in Table 1. No difference was observed between CTV20 and CTV15 groups based on age, sex, tumour side, MGMT methylation, IDH mutation, resection extent (debulking/biopsy), or performance status. There was no difference in GTV volume either, with mean values of 37.8cm3 and 39.7cm3 (p=0.71) for CTV15 and CTV20 groups, respectively. In the CTV15 group, CTV and PTV were reduced from 238.9cm3 to 176.7cm3 (p=0.001) and from 292.6cm3 to 217.0cm3 (p<0.001), respectively. As a result, average brain mean dose (Dmean) and median left hippocampus Dmean were reduced from 25.2Gy to 21.0Gy (p=0.002) and from 43.7Gy to 10.6Gy (p=0.04), respectively. Significantly lower values were also observed for brainstem dose to 0.03cc (D0.03cc), cochleas Dmean and pituitary Dmean. There was no significant difference for other OARs (Table 1). Patient outcome was similar, i.e., median PFS was 8.0 (95% CI: 6.2-9.8) and 7.0 months (95% CI: 6.3-7.7) (p=0.80), and median OS was 11.0 (95% CI: 8.0-14.0) and 14.0 months (95% CI: 11.8-16.2) (p=0.61) for CTV20 and CTV15, respectively.
Conclusion
In GBM patients, reducing the CTV margin from 20mm to 15mm allowed for reduced dose to the surrounding brain structures without compromising outcome. This offers the potential for less treatment toxicity, as well as more room for dose escalation/reirradiation.