Structural cardiac changes in cardiac MRI after SBRT for targets in close proximity to the heart
Maiwand Ahmadsei,
Switzerland
MO-0640
Abstract
Structural cardiac changes in cardiac MRI after SBRT for targets in close proximity to the heart
Authors: Maiwand Ahmadsei1, Bertrand Pouymayou1, Stefanie Ehrbar1, Jochen von Spiczak2, Sebastian M. Christ1, Jonas Willmann1, Boldizsar Kovacs3, Robert Manka4, Ardan M. Saguner3, Matthias Guckenberger1, Nicolaus Andratschke1, Michael Mayinger1
1University Hospital Zurich, Department of Radiation Oncology, Zurich, Switzerland; 2University Hospital Zurich, Diagnostic and Interventional Radiology, Zurich, Switzerland; 3University Hospital Zurich, Department of Cardiology, Zurich, Switzerland; 4University Hospital Zurich, Diagnostic and Interventional Radiology and Department of Cardiology, Zurich, Switzerland
Show Affiliations
Hide Affiliations
Purpose or Objective
Stereotactic body radiation therapy (SBRT) has become a standard of care for early stage non-small cell lung cancer and pulmonary oligometastases. Recent studies indicate that incidental irradiation of the heart is associated with a risk of increased non-cancer deaths. This study aims to assess and examine structural cardiac changes following peri- and epicardial SBRT using a systematic cardiac follow-up protocol including cardiac magnetic resonance (CMR) imaging.
Material and Methods
For 1485 patients treated with local-ablative SBRT from January 2014 to February 2022 at our institution, the distance between the planning target volume (PTV) and the heart was measured. Forty-eight out of 134 patients treated in close proximity (<2cm) to the heart were alive at follow-up. Of those, 20 were randomly invited to undergo a structured cardiac follow-up protocol including CMR, transthoracic echocardiography (TTE), ECG, blood sampling, and two questionnaires, evaluating the quality of life and cardiac symptoms after SBRT, respectively. Ten patients agreed to participate. Registration of CMR image data and the SBRT treatment plan was performed to examine a possible correlation between the dose delivered to the myocardium and structural cardiac changes assessed by CMR. Automated segmentation of 17 heart sub-structures (great vessels, atria, ventricles, coronary arteries, valves, sinoatrial and atrioventricular nodes) was performed for detailed anatomical analysis.
Results
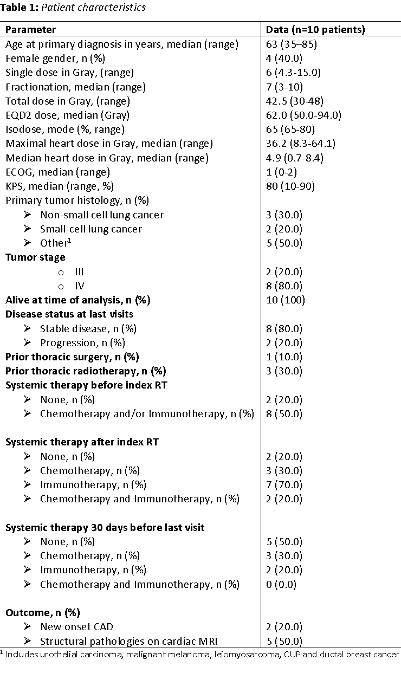
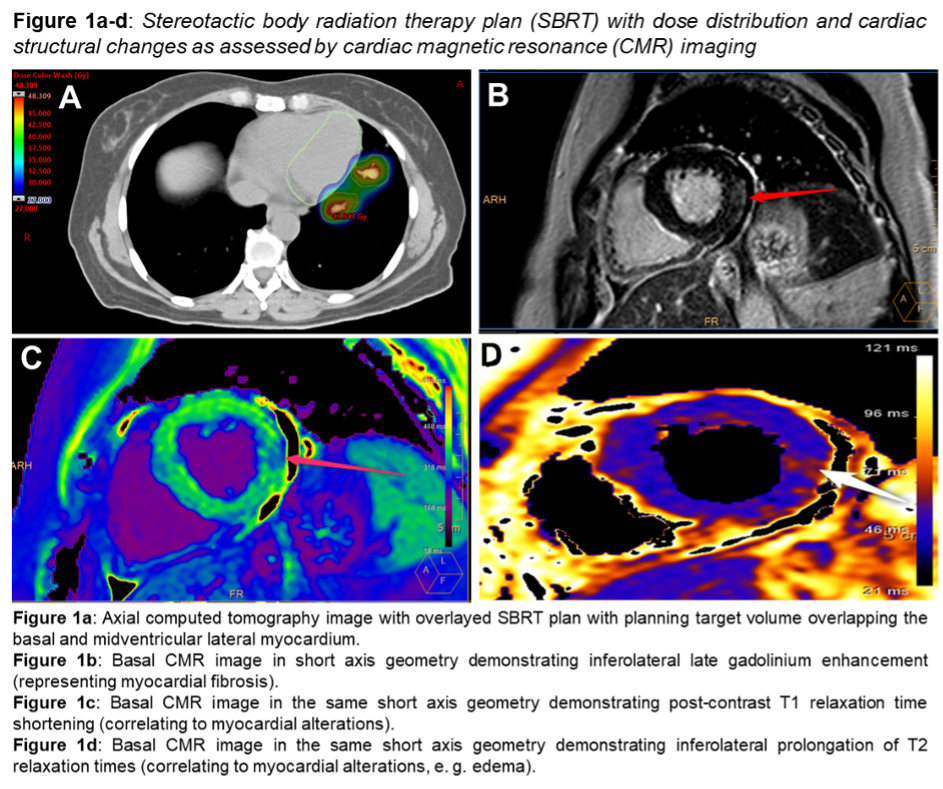
Among the 10 participating patients, the most common primary tumors were non-small cell lung cancer (n=3) and small-cell lung cancer (n=2) (Table 1). Five patients presented with pre-SBRT cardiovascular comorbidities including coronary artery disease and atrial fibrillation. Seven patients received SBRT for pulmonary or vertebral metastases and three patients for primary lung cancer with a median dose of 42.5 Gy (30.0-48.0 Gy) in 3-10 fractions. The mean heart dose (Dmean) and maximum heart dose (Dmax) were 4.9 Gy (0.7-8.4 Gy) and 36.2 Gy (8.3 – 64.1 Gy), respectively. On CMR, five patients showed myocardial alterations, such as fibrosis and edema after a median follow-up time of 5.6 years (0.1-6.3 years). All detected lesions were overlapping or in close proximity to the PTV within the myocardium (Figure 1). Patients with structural changes of the myocardium showed significantly higher Dmax (135.4 Gy vs. 25.4 Gy, p=0.009), Dmean (4.4 Gy vs. 3.4 Gy, p=0.05), D0.1cc (106.3 Gy vs. 21.5 Gy, p=0.006) and D0.03 (117.2 Gy vs. 22.9 Gy, p=0.007). Structural changes on CMR showed a Dmean of 25.9 Gy (21.7-38.3 Gy; EQD2 α/β=3 Gy: 49.4 Gy, 24.8-64.9 Gy) and a Dmax of 40.5 Gy (29.1-61.8 Gy; EQD2 α/β=3 Gy: 110.65 Gy, 38.6-146.2 Gy).
Conclusion
In this pilot-study, 50% of participating patients treated with SBRT for pulmonary targets within 2 cm of the heart showed structural changes of the myocardium in CMR. The presence of structural changes correlates with higher heart doses.