Fast catheter trajectory planning for patient-tailored cervical cancer brachytherapy applicators
Robin Straathof,
The Netherlands
MO-0297
Abstract
Fast catheter trajectory planning for patient-tailored cervical cancer brachytherapy applicators
Authors: Robin Straathof1,2, Sharline van Vliet-Pérez2,1, Inger-Karine Kolkman-Deurloo2, Remi Nout2, Ben Heijmen2, Linda Wauben1, Jenny Dankelman1, Nick van de Berg1
1Delft University of Technology, BioMechanical Engineering, Delft, The Netherlands; 2Erasmus MC Cancer Institute, University Medical Center Rotterdam, Radiotherapy, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Patient-tailored hybrid intracavitary/interstitial (IC/IS) cervical cancer brachytherapy (BT) applicators may aid in improving dose conformity in large tumours or unfavourable anatomies. Several manual or partially automated methods to customise implant configurations have been proposed, but optimality and convergence thereof rely on expertise of the clinician or quality of a small set of a priori specified (straight) dwell segments. Fully automated curved source or catheter channel planning is not yet available. The aim of this work is to introduce and validate a fast approach for generating a large set of feasible catheter trajectories, and selecting sets of optimal configurations that can be integrated in 3D-printed patient-tailored applicators.
Material and Methods
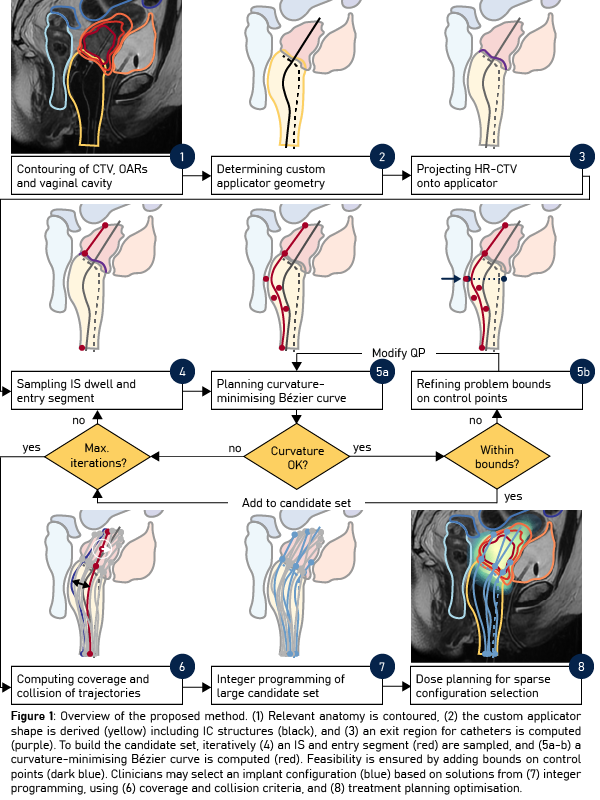
The proposed workflow (Figure 1) was applied retrospectively to generate virtual implant configurations for the first fraction in five patients previously treated with the IC/IS Venezia applicator (Elekta, Stockholm, Sweden). The patient-tailored applicator shape was derived from the distended vaginal geometry and contained existing tandem and lunar ovoids. Additional candidate catheter channels were iteratively planned between straight IS and entry segments. As channels’ centrelines were represented by Bézier curves, i.e. smooth spatial curves defined by a set of control points, minimisation of a channel’s curvature could be formulated as a quadratic program (QP). Non-convex applicator boundary constraints were iteratively refined into QP bounds on the control points to ensure feasibility. Geometric target coverage planning by integer programming was used to compute minimal sets of catheter configurations. Dose plans for Venezia and custom implant configurations were generated using the linear formulation of IPSA.
Results
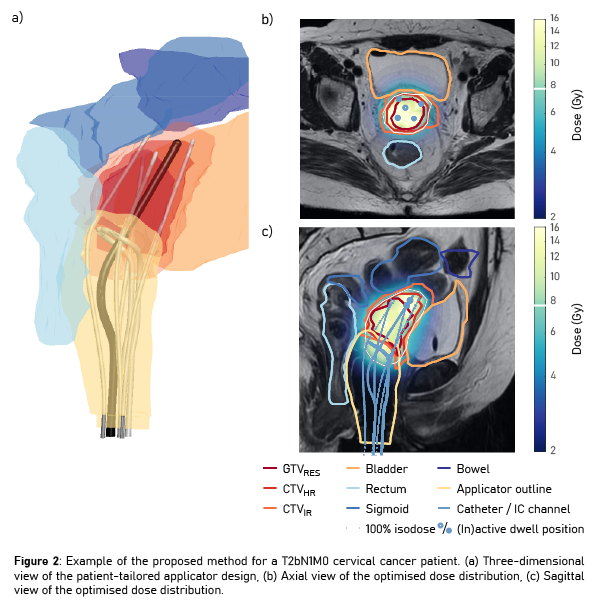
Optimal channel configurations based on hundreds of candidate trajectories were determined within 5 minutes. For all patients a sparse implant configuration could be found that contained the same number of or fewer catheters (median: 4, range: 3-4) than clinically implanted (median: 5, range: 3-6), whilst satisfying all planning constraints (Figure 2). Dosimetric indices were similar for Venezia / patient-tailored applicators; the median (range) D90% of the HR-CTV was 93.1 (90.0-94.8) / 91.9 (90.7-93.8) Gy EQD2, and the D2cm3 of OARs were 77.6 (75.5-78.9) / 77.6 (75.7-79.1), 60.1 (48.8-62.6) / 62.2 (50.9-64.6), and 68.7 (59.4-69.3) / 66.7 (58.3-68.6) Gy EQD2 for bladder, rectum and sigmoid respectively.
Conclusion
The proposed method was shown to be capable of generating BT implant configurations using less catheters than clinically implanted whilst achieving similar dose planning objectives. As the optimisation procedure returns an array of sparse catheter configurations, the user may select a specific configuration and plan that best meets clinical objectives, and potentially reduces the amount of catheters required.