Adaptive brachytherapy for cervical cancer in combined 1.5T MR/HDR suite: Impact of repeated imaging
Katelijne M. van Vliet-van den Ende,
The Netherlands
MO-0296
Abstract
Adaptive brachytherapy for cervical cancer in combined 1.5T MR/HDR suite: Impact of repeated imaging
Authors: Katelijne van Vliet-van den Ende1, Rogier I. Schokker1, Astrid A.C. De Leeuw1, Marinus A. Moerland1, Petra S. Kroon1, Paulien G. Hoogendoorn-Mulder1, Judith M. Roesink1, Raquel Davila Fajardo1, Femke Van der Leij1, Ina M. Jurgenliemk-Schulz1
1UMC Utrecht, Radiotherapy, Utrecht, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
At our department we have a dedicated 1.5 Tesla MRI/HDR brachytherapy suite, which provides the possibility of repeated MRI scanning before, during and after applicator insertion and before and/or after irradiation for advanced cervical cancer patients. This provides insight into intrafraction movement and deformation of organs adjacent to the treatment target and the applicator and allows for interventions when indicated. We analysed this adaptive workflow, and the dosimetric effect of the interventions for the organs at risk (OAR) in order to get a better estimation of the actually delivered dose.
Material and Methods
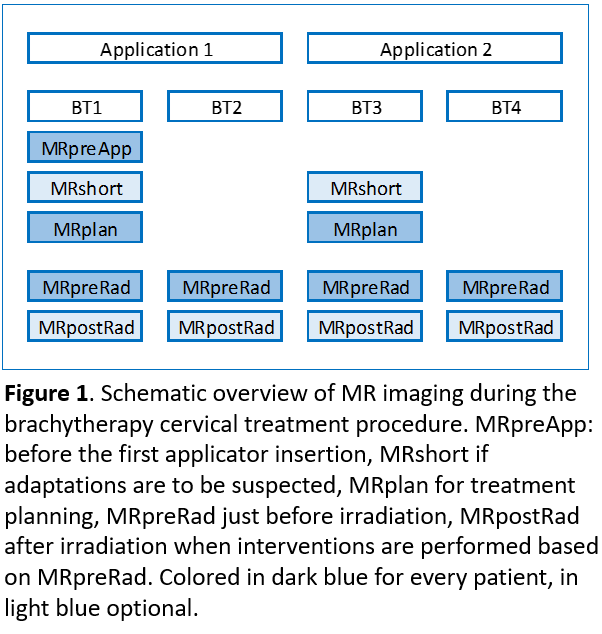
Seventy patients with locally advanced cervical cancer FIGO2009 stages 1B-IVA, treated from June 2016 till August 2020, were retrospectively analysed. Standard schedule consisted of 2 applicator insertions and delivery of 3 or 4 HDR fractions. Repeated MR imaging was performed before and/or after application and before and/or after each HDR fraction (see Figure 1).
Various adaptations were possible, such as replacement of the applicator, adaptation of needle depth, changing the bladder filling to lower the bowel dose or degassing the rectum.
All adaptations were noted and all OAR’s were re-contoured on the repeated MRI scans. The dose differences between total prescribed and total delivered dose for bladder, rectum, sigmoid and bowel were calculated.
For the rectum we analysed the dose effect of the adaptation by contouring the rectum before and after repeated degassing.
Results
In 142 applicator insertions, 92 MRshort, 142 MRplan, 272 MRpreRad and 15 MRpostRad scans were made and analysed. Replacement of the applicator was performed 3 times. Adaptations of needle position based on MRI information was done in 30% of the 79 times needles were inserted. Bladder filling was changed 60 times (42%) before the final MRplan and 14 times (5%) before irradiation. Repeated rectal degassing was done 53 times (19%). After repeated degassing the mean dose difference per fraction for rectum was -1.2 range (-2.9,5) Gy EQD2.
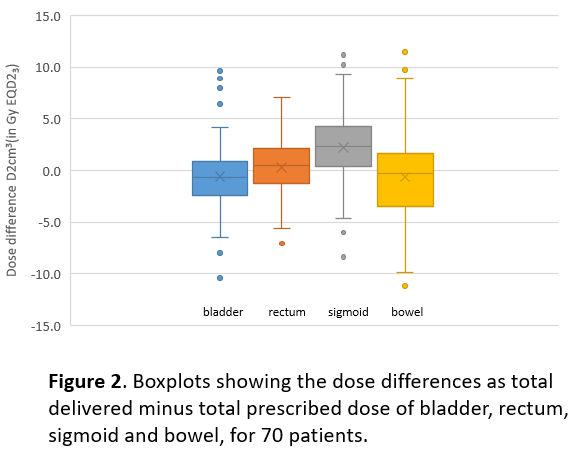
Dose differences between total prescribed and total delivered dose for bladder, rectum, sigmoid and bowel were -0.6 (range -10.4,9.6) Gy EQD2, 0.3 (range -7.1,7.0) Gy EQD2, 2.2 (range -8.3,11.1) Gy EQD2, -0.6 (range -11.2,11.5) Gy EQD2, respectively (Figure 2).
The mean difference between total delivered and prescribed dose has improved for rectum compared to results before our adaptive workflow, while for sigmoid it has increased as its position is difficult to control. For individual patients large differences for OAR doses were found, but this was within the treatment planning doses constraints in the majority of cases.
Conclusion
With an MRI scanner integrated into the brachy suite repeated MRI scanning is possible. This allows for multiple interventions before planning or irradiation and let to a customized, patient centered treatment and better estimation of the real delivered dose.