Prospective assessment of interstitial needles with TRUS in cervical cancer brachytherapy
MO-0298
Abstract
Prospective assessment of interstitial needles with TRUS in cervical cancer brachytherapy
Authors: Johannes Knoth1, Alina Sturdza2, Alexandru Zaharie2, Aleksandra Winkler2, Hannes Sperrer2, Joachim Widder2, Nicole Nesvacil2, Christian Kirisits2, Maximilian P. Schmid2
1Medical University of Vienna, Department of Radiation Oncology, Comprehensive Cancer Center, Vienna, Austria; 2Medical University of Vienna, Department of Radiation Oncology, Comprehensive Cancer Center , Vienna, Austria
Show Affiliations
Hide Affiliations
Purpose or Objective
To prospectively evaluate the visibility (quantitatively and qualitatively) of interstitial needles in cervical cancer patients with combined intracavitary/interstitial (IC/IS) applications using transrectal ultrasound images (TRUS).
Material and Methods
This is a prospective single arm cohort study. Inclusion criteria were (1) treatment with MR-IGABT for cervical cancer and (2) utilization of IC/IS. TRUS (bk5000, BK Medical) was performed during and after applicator insertion and each inserted needle was documented by an axial screenshot on the level of the largest diameter of the high-risk clinical target volume (HR-CTV) for analysis. For qualitative assessment, the visibility of each needle was rated on TRUS with the following scoring system: 0=no visibility, 1=poor discrimination, margin blurred 2=fair discrimination, margin indistinct, 3=excellent discrimination, margin distinct. For quantitative assessment, the distance between the tandem and each needle was measured separately and compared to the respective measurement on MRI. The expected implant quality for optimal dose prescription was rated with the following scoring system: 1=excellent (HR-CTV and organs at risk (OAR’s) soft constraints were met), 2=sufficient (HR-CTV or OAR’s soft constraints violated), 3=poor (HR-CTV and OAR’s soft constraints violated), 4=insufficient (HR-CTV and/or OAR’s hard constraints violated). Evaluation and measurements were performed by 3 radiation oncologists with more than 5 years of experience. Descriptive statistics were used for data analysis.
Results
Patient accrual began in 05/2022. By now, 11 patients with local FIGO stage IIB-IIIB with 20 applications and a total of 112 needles (94 straight through the ring, 12 oblique through the ring, 6 free-handed) were available. Overall, 110/112 needles (98.2%) were visible, mean visibility score ± standard deviation (SD) was 2.6 ± 0.7 for all visible needles. The two non-visible needles (both inserted free-handed) were masked by artefacts or outside the field of view.
Maximum (max), minimum (min), mean ± SD distance of the visible needles to tandem was 35mm, 4mm, 17.4mm ± 4.0mm on MRI and 28 mm, 6 mm, 17.2mm ± 3.4mm on TRUS, respectively. Max and mean ± SD difference between MRI and TRUS was 4 mm, 1.1mm ± 1.0 mm. 3/110 needles (2.7%) had a difference of more than 3mm.
Expected implant quality based on TRUS imaging and actual implant quality after MRI-based planning are compared in table 1.
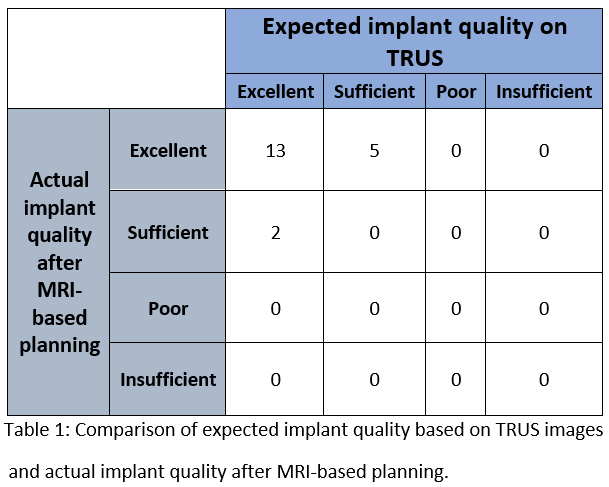
Conclusion
Almost all interstitial needles (98%) were visible on TRUS in this interim analysis. Needles inserted through the predefined applicator positions were always detectable. Qualitatively, the majority of needles showed a distinct signal on TRUS. The quantitative difference compared to MRI was within 3mm in 97%. The expected implant quality based on TRUS imaging was congruent with the actual MRI-based implant quality in the majority of cases. Implant quality was rather underestimated on TRUS in the non-congruent cases.